")
")
Submission of the manuscript is online via e-mail
ecgarticle@gmail.com or
cholerez@mail.ru
Editorial Correspondence e-mail
gastrossr@gmail.com
Publishing, Subscriptions, Sales and Advertising, Correspondence e-mail
journal@cniig.ru
Tel: +7 917 561 9505
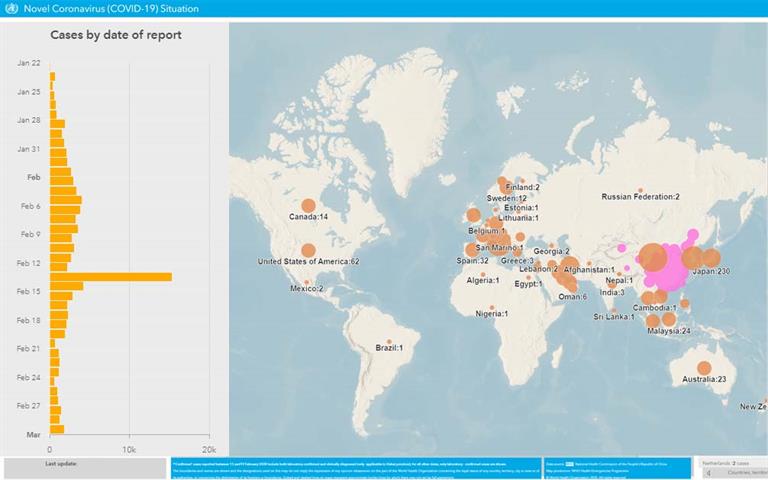
Coronavirus disease (COVID-19) Situation dashboard
This interactive dashboard/map provides the latest global numbers and numbers by country of COVID-19 cases on a daily basis.
№ 01 (137) 2017
-
Надеемся на продолжение нашего сотрудничества. Уважаемые коллеги !
Уважаемые коллеги !
Оставаясь верными сложившимся традициям, Новый 2017 год мы открываем журнал «Экспериментальная и клиническая гастроэнтерология», входящий в список, рекомендуемый ВАК, и цитируемый системами РИНЦ и Scopus, номером, посвященным заболеваниям желудочно-кишечного тракта в детском возрасте. Поскольку формирование не только заболеваний ЖКТ, а и предрасположенности к ним происходит в самом раннем периоде детства, открывается номер статьей группы авторов под руководством мэтра отечественной физиологии Г. Ф. Коротько, которые в результате собственных исследований пришли к заключению о том, что содержание гидролитических ферментов в околоплодных водах, содержимом желудка и сыворотке крови пуповины, их изменения при неполных сроках гестации обладают диагностической информативностью в оценке дигестивного потенциала новорожденного.
Продолжает эту тему оригинальная работа авторов из Ташкентского Педиатрического Медицинского Института с выводом о том, что дефицит биоэлементов является частой причиной серьезных нарушений функционирования органов и систем, внутриутробной задержки развития плода, анемии, что приводит к рождению детей с малым весом и увеличению заболеваемости в неонатальном периоде. Изложены наиболее частые причины дефицита и избытка макро- и микроэлементов, выделены группы риска по развитию недостаточности микроэлементов.
Следующая работа от исследователей из Первого МГМУ им. И. М. Сеченова в разделе «Клиническая гастроэнтерология» посвящена особенностям пищевода Барретта у детей. Сделан важный вывод о том, что длительное течение эзофагита, эрозивный эзофагит, патологический кислотный ГЭР предрасполагают к развитию у детей пищевода Барретта при отсутствии достоверных клинических особенностей течения.
Целый кластер оригинальных работ поднимает проблему нарушения микробиоты кишечника у детей и его влияния на течение функциональный расстройств. Наши коллеги из Санкт-Петербурга выявили, что среди детей с СИБР достоверно чаще встречалась функциональная диспепсия, лактазная недостаточность. При этом клиническая картина СИБР у детей оказалась неспецифична, однако пробиотическая терапия оказывала выраженный терапевтический эффект.
В следующей статье учеными из Перми на основании путем применения соответствующего математического аппарата создана модель прогнозирования развития тяжелых форм ротавирусной инфекции (РВИ) у госпитализированных детей раннего возраста. В качестве прогностического критерия предлагается использовать коэффициент позитивности (КП), вычисляемый при проведении иммуноферментного анализа (ИФА) тест-системы «Ротавирус-антиген-ИФА-БЕСТ» (г. Новосибирск) в первые сутки госпитализации. Разработан алгоритм определения порогового разделяющего значения коэффициента. Определена вероятность развития тяжелых форм РВИ у детей раннего возраста, в 3,5 раза превышающая показатель, установленный клинически. С учетом результата ИФА из фекалий ребенка в первый день госпитализации определен прогноз вероятности тяжелой формы РВИ, который может служить обоснованием ранней терапии иммуноглобулинами для внутривенного введения.
Отдел кишечных инфекций ФГБУ Научно-исследовательского института детских инфекций Федерального медико-биологического агентства России наблюдал 143 пациента в возрасте от 1 до 7 лет, без гастроэнтерологической патологии в анамнезе со среднетяжелой ротавирусной (РВИ), норовирусной (НВИ) и смешанной ротаноровирусной (РНВИ) кишечными инфекциями, верифицированными методом ПЦР в фекалиях. В результате в остром периоде РВИ обнаружено достоверное снижение Bacteroides thetaiataomicron. и увеличение Bacteroides fragilis по сравнению с НВИ. Пролиферация УПМ отмечалась у четверти больных ВКИ и сопровождалась воспалительными изменениями в копрограмме, более часто при РНВИ. Сделан вывод, что дисбиоз кишечника и СИБР при ВКИ патогенетически связаны с развитием постинфекционной функциональной патологии органов пищеварения у детей. В следующей статье авторы из ФГАУ «Научный центр здоровья детей» Министерства здравоохранения Российской Федерации напоминают нам, что тирозинемия I типа — это редкое генетическое заболевание, приводящее к развитию цирроза печени, печеночной недостаточности и тубулопатии. В связи с этим огромное значение имеет ранняя диагностика и своевременное начало патогенетического лечения заболевания. Ученые из Нижегородской медицинской академии, Первого МГМУ им. И. М. Сеченова и Северо-западного государственного медицинского университета им И. И. Мечникова изучали уровень гастрина сыворотки крови у детей при лёгкой форме гепатита В, его влияние на клиническое течение болезни. Сделан вывод о том, что желтушные формы гепатита В у детей, начиная с легкой формы болезни, в большинстве случаев сопровождается функциональной диспепсией. Диспансерное наблюдение и реабилитацию детей, перенесших желтушные формы ГВ, начиная с лёгкой формы болезни, врачу-инфекционисту необходимо проводить совместно с врачом-гастроэнтерологом; это обеспечит своевременное выявление у них гастродуоденальной патологии и положительно повлияет на увеличение доли здоровых детей.
Раздел «Обзоры» представлен материалом А. И. Хавкина и О. Н. Комаровой из РНИМУ им. Н. И. Пирогова (Москва) о болезни Вольмана или дефиците кислой лизосомальной липазы — редком аутосомно-рецессивном заболевании, вызванном повреждающими мутациями гена LIPA.
Наш традиционный раздел «Лекции» будет интересен врачам всех специальностей, так как в Российской Федерации проблема пищевой анафилаксии, возникающей при употреблении рыбы, у детей освещается крайне скудно и данные о её распространенности до настоящего времени отсутствовали.
Завершает номер наша постоянная рубрика «Клинические наблюдения», в которой представлены два случая аллергической энтеропатии у 4‑летнего ребенка с целиакией и у новорожденного недоношенного ребенка. Оба наблюдения весьма интересны ввиду растущей частоты аллергической патологии и глютен ассоциированных заболеваний.
Ждем от вас интересных стаей, клинических случаев. И желаем приятного и полезного прочтения.
Ответственная за выпуск,Заведующая кафедрой пропедевтики
детских болезней педиатрического факультета
ФГБОУ ВО Первый Московский государственный
медицинский университет им. И. М. Сеченова
доктор медицинских наук, профессорС. И. Эрдес
-
- Государственное бюджетное учреждение здравоохранения «Краевая клиническая больница № 2» министерства здравоохранения Краснодарского края (Краснодар, Россия)
Ключевые слова:околоплодные воды,гидролазы,пепсиногены,недоношенность,задержка развития плода,молочное вскармливание
Резюме:Цель исследования: установление возможности характеристики дигестивного потенциала новорожденных по содержанию гидролаз пищеварительных желез в околоплодных водах, сопоставлению его с одноименными ферментативными активностями сыворотки пуповинной и венозной материнской крови, содержимого желудка новорожденного. Материалы и методы: по согласованию с родителями, в родах у 76 родильниц (40 имели доношенную и 36 недоношенную беременность) получены околоплодные воды, взяты пробы крови пуповины новорожденного, его желудочного содержимого, венозной крови матери. Стандартными методами определены липаза, α-амилаза, щелочная фосфатаза, пепсиноген I и пепсиноген II. Результаты обработаны методами непараметрической статистики. Результаты: оценка дигестивного ферментного потенциала системы пищеварения новорожденных может быть произведена путем определения гидролитических ферментов во взятых в родах околоплодных водах, так как их гидролазы и зимогены в конце гестации имеют фетальное происхождение. При недоношенной беременности и задержке внутриутробного развития плода концентрация гидролаз и пепсиногенов пищеварительных желез в околоплодных водах, содержимом желудка и сыворотке пуповинной крови снижена, что повышает вероятность диспепсии новорожденного. Заключение: содержание гидролитических ферментов в околоплодных водах, содержимом желудка и сыворотке крови пуповины, их изменения при неполных сроках гестации позволяют заключить о их диагностической информативности в оценке дигестивного потенциала новорожденного.
-
- Володин Н. Н. (гл. ред.) Неонатология. Национальное руководство // М.: ГЕОТАР-Медиа, 2007. 848 с.
- Конь И. Я. Основы естественного вскармливания детей первого года жизни / И. Я. Конь, М. В. Гмошинская, Е. М. Фатеева // Тутелян В. А., Конь И. Я. Детское питание. Руководство для врачей, 2009. Ч. II, гл. 1. С. 277 - 339.
- Шабалов Н. П. (гл. ред.) Неонатология - 4-е изд. [В 2-х т.]. М.: МЕДпресс-информ, 2006. 344 с.
- Адамкин Дэвид Х. Стратегия питания младенцев с очень низкой массой тела при рождении. Пер. с англ., под ред. Е. Н. Байбариной. М.: Изд. группа «ГЭОТАР-Медиа», 2013. 776 с.
- Коротько Г. Ф. Питание и пищеварение на ранних этапах онтогенеза человека. Краснодар: «Традиция», 2016. 88 с.
- Халафян А. А. STATISTICA 6. Математическая статистика с элементами теории вероятностей. Учебник. - М.: Издательство Бином, 2010. - 496 с.
- Колодкина Е. В., Камакин Н. Ф. Ферментный гомеостаз у женщин при беременности в зависимости от срока и вида родоразрешения. Киров: Кировская ГМА, 2008. 111 с.
- Ширина Л. И., Мазо В. К. Система пищеварения ребенка, ее созревание // Тутелян В. А., Конь И. Я. Детское питание. Руководство для врачей, 2009. Ч. I, гл. 3. С. 25 - 50.
- Уголев А. М. Эволюция пищеварения и принципы эволюции функций. Элементы современного функционализма. Л.: Наука, 1985. 544 с.
- Харькова Р. М. Кислотность желудочного сока и активность пепсина у детей первого года жизни при различных видах пищи // Вопросы питания. 1969. Т. 28, № 1. С. 43 - 49.
- Закс М. Г., Никитин В. Н. Онтогенез пищеварительной функции. Возрастная физиология // Руководство по физиологии. Л.: Наука, 1975. С. 263 - 312.
- Клиорин А. И. Некоторые возрастные особенности функций желудочно-кишечного тракта у детей // Справочник по детской диететике (ред. И. М. Воронцов, А. В. Мазурин). Л.: Медицина, 1977. С. 5 - 11.
Опубликовано :
КОМПЛЕКСНАЯ ОЦЕНКА ДИГЕСТИВНОГО ФЕРМЕНТНОГО ПОТЕНЦИАЛА НОВОРОЖДЕННОГО. Экспериментальная и клиническая гастроэнтерология. 2017;137(01):03-07
Загрузить полный текст
-
- СЗГМУ им. И. И. Мечникова, Санкт-Петербург (Санкт-Петербург, Россия)
- Гос. НИИ ОЧБ ФМБА России (Санкт-Петербург, Россия)
- Институт экспериментальной медицины (Санкт-Петербург, Россия)
- ПСПбГМУ им. акад. И. П. Павлова (Санкт-Петербург, Россия)
Ключевые слова:бутират,дисбиоз толстой кишки,микробиота кишечника,целиакия,язвенный колит
Резюме:Цель исследования: изучить количественный состав некоторых представителей симбиотической микробиоты толстой кишки и выявить особенности дисбиоза кишечника у пациентов с язвенным колитом и целиакией. Материалы и методы: В исследование было включено 40 пациентов с активным язвенным колитом (легкая и среднетяжелая атаки), получающих терапию препаратами месалазина, 43 пациента с целиакией, находящихся на безглютеновой диете, и 42 практически здоровых добровольца. Для количественного определения микроорганизмов ДНК, выделенную из образцов кала, подвергали полимеразной цепной реакции (ПЦР) в режиме реального времени. Результаты: У пациентов с язвенным колитом, как и у больных целиакией, количество Faecalibacterium prausnitzii было значимо меньше, чем у здоровых лиц (p = 0,043 и p = 0,036 соответственно). Общее количество бутират-продуцирующих бактерий, имеющих ген бутирил-КоA: ацетат-КоA-трансферазы (but), было снижено (по сравнению со здоровыми добровольцами) только у пациентов с язвенным колитом (p = 0,048). Несмотря на то, что общее количество бактероидов между группами пациентов не различалось, Bacteroides thetaiotaomicron существенно реже встречался у пациентов с язвенным колитом, чем у здоровых лиц (p = 0,016). Отсутствие Bacteroides thetaiotaomicron в кале или его уровень ниже порога обнаружения были значимо связаны с язвенным колитом (ОШ = 6,30; 95% ДИ: 1,33 - 29,95). У пациентов с целиакией уровень Bifidobacterium spp. был значимо снижен по сравнению как со здоровыми добровольцами, так и с больными язвенным колитом (p = 0,022 и p = 0,046 соответственно). Как при язвенном колите, так и при целиакии таксономический дисбиоз характеризовался повышенным отношением Bacteroides fragilis spp. к Faecalibacterium prausnitzii по сравнению со здоровыми лицами (p < 0,05 в обоих случаях). Выводы: Повышенное отношение Bacteroides fragilis к Faecalibacterium prausnitzii может рассматриваться в качестве потенциального биомаркера дисбиоза кишечника провоспалительного типа. Уменьшение численности бутират-продуцирующих бактерий подтверждает целесообразность восполнения дефицита масляной кислоты при обоих заболеваниях путем дополнительного назначения препаратов масляной кислоты, пробиотиков на основе бутират-продуцирующих бактерий, бутирогенных пребиотиков и метабиотиков. Bacteroides thetaiotaomicron может играть защитную роль в организме человека, возможно, предохраняя его от развития воспалительных заболеваний кишечника. Снижение уровня Bifidobacterium spp. у пациентов с целиакией может свидетельствовать о защитной функции некоторых видов бифидобактерий и целесообразности применения пробиотиков на основе бифидобактерий и пребиотиков инулинового типа.
-
- Lederberg J. Infectious history. Science. 2000 Apr 14;288 (5464):287 - 293.
- Nicholson JK, Holmes E, Lindon JC, Wilson ID. The challenges of modeling mammalian biocomplexity. Nat Biotechnol. 2004 Oct; 22 (10):1268 - 74.
- Goodacre R. Metabolomics of a superorganism. J Nutr. 2007 Jan; 137 (1 Suppl):259S-266S.
- Rosenberg E, Sharon G, Zilber-Rosenberg I. The hologenome theory of evolution contains Lamarckian aspects within a Darwinian framework. Environ Microbiol. 2009 Dec; 11 (12):2959 - 62.
- Sleator R. D. The human superorganism - of microbes and men. Med Hypotheses. 2010 Feb; 74 (2):214 - 5.
- van Duynhoven J, Vaughan EE, Jacobs DM, Kemperman RA, van Velzen EJ, Gross G, Roger LC, Possemiers S, Smilde AK, Doré J, Westerhuis JA, Van de Wiele T. Metabolic fate of polyphenols in the human superorganism. Proc Natl Acad Sci U S A. 2011 Mar 15;108 Suppl 1:4531 - 8.
- Gill SR, Pop M, Deboy RT, Eckburg PB, Turnbaugh PJ, Samuel BS, Gordon JI, Relman DA, Fraser-Liggett CM, Nelson KE. Metagenomic analysis of the human distal gut microbiome. Science. 2006 Jun 2;312 (5778):1355 - 9.
- Qin J, Li R, Raes J, Arumugam M, Burgdorf KS, Manichanh C, Nielsen T, Pons N, Levenez F, Yamada T, Mende DR, Li J, Xu J, Li S, Li D, Cao J, Wang B, Liang H, Zheng H, Xie Y, Tap J, Lepage P, Bertalan M, Batto JM, Hansen T, Le Paslier D, at all human gut microbial gene catalogue established by metagenomic sequencing. Nature. 2010 Mar 4;464 (7285):59 - 65.
- Bäckhed F, Fraser CM, Ringel Y, Sanders ME, Sartor RB, Sherman PM, Versalovic J, Young V, Finlay BB. Defining a healthy human gut microbiome: current concepts, future directions, and clinical applications. Cell Host Microbe. 2012 Nov 15;12 (5):611 - 22. doi: 10.1016/j. chom. 2012.10.012.
- Rajilić-Stojanović M, de Vos WM. The first 1000 cultured species of the human gastrointestinal microbiota. FEMS Microbiol Rev. 2014 Sep; 38 (5):996 - 1047. doi: 10.1111/1574 - 6976.12075.
- Harmsen HJ, de Goffau MC. The Human Gut Microbiota. Adv Exp Med Biol. 2016;902:95 - 108. doi: 10.1007/978-3-319-31248-4_7.
- Guarner F, Malagelada JR. Gut flora in health and disease. Lancet. 2003 Feb 8;361 (9356):512 - 9.
- Guarnier F. The enteric microbiota. In: Granger DN, Granger J, Morgan & Claypool Life Sciences, eds. Colloquium Series on Integrated Systems Physiology: From Molecule to Function to Disease. USA: Morgan & Clay pool Life Sciences Publishers, 2011: 1 - 77.
- Prakash S, Rodes L, Coussa-Charley M, Tomaro-Duchesneau C. Gut microbiota: next frontier in understanding human health and development of biotherapeutics. Biologics. 2011;5:71 - 86. doi: 10.2147/BTT. S19099. Epub 2011 Jul 11.
- Sekirov I, Russell SL, Antunes LC, Finlay BB. Gut microbiota in health and disease. Physiol Rev. 2010 Jul; 90 (3):859 - 904.
- Guinane CM, Cotter PD. Role of the gut microbiota in health and chronic gastrointestinal disease: understanding a hidden metabolic organ. Therap Adv Gastroenterol. 2013 Jul; 6 (4):295 - 308. doi: 10.1177/1756283X13482996.
- Philpott H, Gibson P, Thien F. Irritable bowel syndrome - An inflammatory disease involving mast cells. Asia Pac Allergy. 2011 Apr; 1 (1):36 - 42.
- Clarke G., Grenham S, Scully P, Fitzgerald P, Moloney RD, Shanahan F, Dinan TG, Cryan JF. The microbiome-gut-brain axis during early life regulates the hippocampal serotonergic system in a sex-dependent manner. Mol Psychiatry. 2013 Jun; 18 (6):666 - 73.
- Kennedy P. J., Cryan JF, Dinan TG, Clarke G. Irritable bowel syndrome: a microbiome-gut-brain axis disorder? World J Gastroenterol. 2014 Oct 21;20 (39):14105 - 25.
- DuPont AW, DuPont HL. The intestinal microbiota and chronic disorders of the gut. Nat Rev Gastroenterol Hepatol. 2011 Aug 16;8 (9):523 - 31. doi: 10.1038/nrgastro. 2011.133.
- Sartor RB. Gut microbiota: Diet promotes dysbiosis and colitis in susceptible hosts. Nat Rev Gastroenterol Hepatol. 2012 Oct; 9 (10):561 - 2. doi: 10.1038/nrgastro. 2012.157.
- Quigley EM, Monsour HP. The Gut Microbiota and Nonalcoholic Fatty Liver Disease. Semin Liver Dis. 2015 Aug; 35 (3):262 - 9. doi: 10.1055/s-0035 - 1562946.
- Keren N, Konikoff FM, Paitan Y, Gabay G, Reshef L, Naftali T, Gophna U. Interactions between the intestinal microbiota and bile acids in gallstones patients. Environ Microbiol Rep. 2015 Dec; 7 (6):874 - 80. doi: 10.1111/1758 - 2229.12319.
- Verdu EF, Galipeau HJ, Jabri B. Novel players in coeliac disease pathogenesis: role of the gut microbiota. Nat Rev Gastroenterol Hepatol. 2015 Sep; 12 (9):497 - 506. doi: 10.1038/nrgastro. 2015.90.
- Marasco G, Di Biase AR, Schiumerini R, Eusebi LH, Iughetti L, Ravaioli F, Scaioli E, Colecchia A, Festi D. Gut Microbiota and Celiac Disease. Dig Dis Sci. 2016 Jun; 61 (6):1461 - 72. doi: 10.1007/s10620-015-4020-2.
- Hering NA, Fromm M, Schulzke JD. Determinants of colonic barrier function in inflammatory bowel disease and potential therapeutics. J Physiol. 2012 Mar 1;590 (Pt 5):1035 - 44. doi: 10.1113/jphysiol. 2011.224568.
- Neurath MF. Cytokines in inflammatory bowel disease. Nat Rev Immunol. 2014 May; 14 (5):329 - 42. doi: 10.1038/nri3661.
- Круис В., Ситкин С. И. Заживление слизистой оболочки при воспалительных заболеваниях кишечника: Влияние месалазина и различных механизмов его действия на заживление слизистой оболочки кишечника при язвенном колите. - М.: Форте принт, 2013. - 36 с.
- Fujita H, Eishi Y, Ishige I, Saitoh K, Takizawa T, Arima T, Koike M. Quantitative analysis of bacterial DNA from Mycobacteria spp., Bacteroides vulgatus, and Escherichia coli in tissue samples from patients with inflammatory bowel diseases. J Gastroenterol. 2002;37 (7):509 - 16.
- Fallone CA, Bitton A. Is IBD caused by a Helicobacter pylori infection? Inflamm Bowel Dis. 2008 Oct; 14 Suppl 2: S37-8. doi: 10.1002/ibd. 20552.
- Lidar M, Langevitz P, Shoenfeld Y. The role of infection in inflammatory bowel disease: initiation, exacerbation and protection. Isr Med Assoc J. 2009 Sep; 11 (9):558 - 63.
- Hansen R, Thomson JM, El-Omar EM, Hold GL. The role of infection in the aetiology of inflammatory bowel disease. J Gastroenterol. 2010 Mar; 45 (3):266 - 76. doi: 10.1007/s00535-009-0191-y.
- Timms VJ, Daskalopoulos G, Mitchell HM, Neilan BA. The Association of Mycobacterium avium subsp. paratuberculosis with Inflammatory Bowel Disease. PLoS One. 2016 Feb 5;11 (2):e0148731. doi: 10.1371/journal. pone. 0148731.
- Пак С. Г., Малов В. А., Горобченко А. Н. Инфекционные болезни: расширяя традиционные представления // Терапевтический архив. - 2003. - Том 75, № 11. - С. 5 - 10.
- Friswell M, Campbell B, Rhodes J. The role of bacteria in the pathogenesis of inflammatory bowel disease. Gut Liver. 2010 Sep; 4 (3):295 - 306. doi: 10.5009/gnl. 2010.4.3.295.
- Mann EA, Saeed SA. Gastrointestinal infection as a trigger for inflammatory bowel disease. Curr Opin Gastroenterol. 2012 Jan; 28 (1):24 - 9. doi: 10.1097/MOG. 0b013e32834c453e.
- Шкарин В. В., Ковалишена О. В. Вопросы этиологии новых инфекций // Медицина в Кузбассе. - 2013. - Том 12, № 2. - С. 13 - 21.
- Miner-Williams WM, Moughan PJ. Intestinal barrier dysfunction: implications for chronic inflammatory conditions of the bowel. Nutr Res Rev. 2016 Jun; 29 (1):40 - 59. doi: 10.1017/S0954422416000019.
- Macfarlane S, Furrie E, Cummings JH, Macfarlane GT. Chemotaxonomic analysis of bacterial populations colonizing the rectal mucosa in patients with ulcerative colitis. Clin Infect Dis. 2004 Jun 15;38 (12):1690 - 9.
- Frank DN, Robertson CE, Hamm CM, Kpadeh Z, Zhang T, Chen H, Zhu W, Sartor RB, Boedeker EC, Harpaz N, Pace NR, Li E. Disease phenotype and genotype are associated with shifts in intestinal-associated microbiota in inflammatory bowel diseases. Inflamm Bowel Dis. 2011 Jan; 17 (1):179 - 84. doi: 10.1002/ibd. 21339.
- Duboc H, Rajca S, Rainteau D, Benarous D, Maubert MA, Quervain E, Thomas G, Barbu V, Humbert L, Despras G, Bridonneau C, Dumetz F, Grill JP, Masliah J, Beaugerie L, Cosnes J, Chazouillères O, Poupon R, Wolf C, Mallet JM, Langella P, Trugnan G, Sokol H, Seksik P. Connecting dysbiosis, bile-acid dysmetabolism and gut inflammation in inflammatory bowel diseases. Gut. 2013 Apr; 62 (4):531 - 9. doi: 10.1136/gutjnl-2012 - 302578.
- Kabeerdoss J, Sankaran V, Pugazhendhi S, Ramakrishna BS. Clostridium leptum group bacteria abundance and diversity in the fecal microbiota of patients with inflammatory bowel disease: a case-control study in India. BMC Gastroenterol. 2013 Jan 26;13:20. doi: 10.1186/1471-230X-13 - 20.
- Rajilić-Stojanović M, Shanahan F, Guarner F, de Vos WM. Phylogenetic analysis of dysbiosis in ulcerative colitis during remission. Inflamm Bowel Dis. 2013 Mar; 19 (3):481 - 8. doi: 10.1097/MIB. 0b013e31827fec6d.
- Kostic AD, Xavier RJ, Gevers D. The microbiome in inflammatory bowel disease: current status and the future ahead. Gastroenterology. 2014 May; 146 (6):1489 - 99. doi: 10.1053/j. gastro. 2014.02.009.
- Matsuoka K, Kanai T. The gut microbiota and inflammatory bowel disease. Semin Immunopathol. 2015 Jan; 37 (1):47 - 55. doi: 10.1007/s00281-014-0454-4.
- Fukata M, Arditi M. The role of pattern recognition receptors in intestinal inflammation. Mucosal Immunol. 2013 May; 6 (3):451 - 63. doi: 10.1038/mi. 2013.13.
- Swidsinski A, Loening-Baucke V, Herber A. Mucosal flora in Crohn’s disease and ulcerative colitis - an overview. J Physiol Pharmacol. 2009 Dec; 60 Suppl 6:61 - 71.
- Chen SJ, Liu XW, Liu JP, Yang XY, Lu FG. Ulcerative colitis as a polymicrobial infection characterized by sustained broken mucus barrier. World J Gastroenterol. 2014 Jul 28;20 (28):9468 - 75. doi: 10.3748/wjg. v20.i28.9468.
- Sartor RB, Wu GD. Roles for Intestinal Bacteria, Viruses, and Fungi in Pathogenesis of Inflammatory Bowel Diseases and Therapeutic Approaches. Gastroenterology. 2016 Oct 18. pii: S0016-5085 (16) 35235 - 0. doi: 10.1053/j. gastro. 2016.10.012.
- Ситкин С. И., Ткаченко Е. И., Вахитов Т. Я. Метаболический дисбиоз кишечника и его биомаркеры // Экспериментальная и клиническая гастроэнтерология. - 2015. - № 12 (124). - С. 6 - 29.
- Huda-Faujan N, Abdulamir AS, Fatimah AB, Anas OM, Shuhaimi M, Yazid AM, Loong YY. The impact of the level of the intestinal short chain fatty acids in inflammatory bowel disease patients versus healthy subjects. Open Biochem J. 2010 May 13;4:53 - 8. doi: 10.2174/1874091X01004010053.
- Selmer T, Andrei PI. p-Hydroxyphenylacetate decarboxylase from Clostridium difficile. A novel glycyl radical enzyme catalysing the formation of p-cresol. Eur J Biochem. 2001 Mar; 268 (5):1363 - 72.
- Marquet P, Duncan SH, Chassard C, Bernalier-Donadille A, Flint HJ. Lactate has the potential to promote hydrogen sulphide formation in the human colon. FEMS Microbiol Lett. 2009 Oct; 299 (2):128 - 34. doi: 10.1111/j. 1574 - 6968.2009.01750.x.
- Rowan FE, Docherty NG, Coffey JC, O’Connell PR. Sulphate-reducing bacteria and hydrogen sulphide in the aetiology of ulcerative colitis. Br J Surg. 2009 Feb; 96 (2):151 - 8. doi: 10.1002/bjs. 6454.
- Tannahill GM, Curtis AM, Adamik J, Palsson-McDermott EM, McGettrick AF, Goel G, Frezza C, Bernard NJ, Kelly B, Foley NH, Zheng L, Gardet A, Tong Z, Jany SS, Corr SC, Haneklaus M, Caffrey BE, Pierce K, Walmsley S, Beasley FC, Cummins E, Nizet V, Whyte M, Taylor CT, Lin H, Masters SL, Gottlieb E, Kelly VP, Clish C, Auron PE, Xavier RJ, O’Neill LA. Succinate is an inflammatory signal that induces IL-1β through HIF-1α. Nature. 2013 Apr 11;496 (7444):238 - 42. doi: 10.1038/nature11986.
- Ситкин С. И., Ткаченко Е. И., Вахитов Т. Я., Орешко Л. С., Жигалова Т. Н. Метаболом сыворотки крови по данным газовой хроматографии - масс-спектрометрии (ГХ-МС) у пациентов с язвенным колитом и больных целиакией // Экспериментальная и клиническая гастроэнтерология. - 2013. - № 12. - С. 44 - 57.
- Sitkin S., Vakhitov T., Tkachenko E., Oreshko L., Zhigalova T. Metabolic dysbiosis concept and its biomarkers in ulcerative colitis and celiac disease. J Crohns Colitis. 2015;9 (Suppl 1):S437. doi: 10.1093/ecco-jcc/jju027.829.
- Корниенко Е. А. Роль кишечной микробиоты в развитии целиакии // Медицинский совет. - 2013. - № 1. - С. 44 - 51.
- De Palma G, Nadal I, Collado MC, Sanz Y. Effects of a gluten-free diet on gut microbiota and immune function in healthy adult human subjects. Br J Nutr. 2009 Oct; 102 (8):1154 - 60. doi: 10.1017/S0007114509371767.
- Brown K, DeCoffe D, Molcan E, Gibson DL. Diet-induced dysbiosis of the intestinal microbiota and the effects on immunity and disease. Nutrients. 2012 Aug; 4 (8):1095 - 119. doi: 10.3390/nu4081095.
- Golfetto L, de Senna FD, Hermes J, Beserra BT, França Fda S, Martinello F. Lower bifidobacteria counts in adult patients with celiac disease on a gluten-free diet. Arq Gastroenterol. 2014 Apr-Jun; 51 (2):139 - 43.
- Ситкин С. И., Ткаченко Е. И., Вахитов Т. Я., Орешко Л. С., Жигалова Т. Н., Авалуева Е. Б. Метаболом сыворотки крови и микробиота кишечника при язвенном колите и целиакии // Вестник Северо-Западного государственного медицинского университета им. И. И. Мечникова. - 2014. - Том 6, № 3. - С. 12 - 22.
- Lorenzo Pisarello MJ, Vintiñi EO, González SN, Pagani F, Medina MS. Decrease in lactobacilli in the intestinal microbiota of celiac children with a gluten-free diet, and selection of potentially probiotic strains. Can J Microbiol. 2015 Jan; 61 (1):32 - 7. doi: 10.1139/cjm-2014 - 0472.
- Di Cagno R, Rizzello CG, Gagliardi F, Ricciuti P, Ndagijimana M, Francavilla R, Guerzoni ME, Crecchio C, Gobbetti M, De Angelis M. Different fecal microbiotas and volatile organic compounds in treated and untreated children with celiac disease. Appl Environ Microbiol. 2009 Jun; 75 (12):3963 - 71. doi: 10.1128/AEM. 02793 - 08.
- Di Cagno R, De Angelis M, De Pasquale I, Ndagijimana M, Vernocchi P, Ricciuti P, Gagliardi F, Laghi L, Crecchio C, Guerzoni ME, Gobbetti M, Francavilla R. Duodenal and faecal microbiota of celiac children: molecular, phenotype and metabolome characterization. BMC Microbiol. 2011 Oct 4;11:219. doi: 10.1186/1471-2180-11-219.
- Calabrò A, Gralka E, Luchinat C, Saccenti E, Tenori L. A metabolomic perspective on coeliac disease. Autoimmune Dis. 2014;2014:756138. doi: 10.1155/2014/756138.
- Sitkin S., Tkachenko E., Oreshko L. Serum metabolome in celiac disease is influenced by gut microbiota // Abstracts of the Falk Symposium 193 «Celiac Disease and Other Small Bowel Disorders» (Amsterdam, The Netherlands, September 5 - 6, 2014). - 2014. - Poster Abstract 95.
- Всероссийский консенсус по диагностике и лечению целиакии у детей и взрослых / Парфенов А. И., Маев И. В., Баранов А. А., Бакулин И. Г., Сабельникова Е. А., Крумс Л. М., Бельмер С. В., Боровик Т. Э., Захарова И. Н., Дмитриева Ю. А., Рославцева Е. А., Корниенко Е. А., Хавкин А. И., Потапов А. С., Ревнова М. О., Мухина Ю. Г., Щербаков П. Л., Федоров Е. Д., Белоусова Е. А., Халиф И. Л., и др. // Альманах клинической медицины. - 2016; 44 (6): 661 - 688.
- de Sousa Moraes LF, Grzeskowiak LM, de Sales Teixeira TF, Gouveia Peluzio Mdo C. Intestinal microbiota and probiotics in celiac disease. Clin Microbiol Rev. 2014 Jul; 27 (3):482 - 9. doi: 10.1128/CMR. 00106 - 13.
- Schroeder KW, Tremaine WJ, Ilstrup DM. Coated oral 5-aminosalicylic acid therapy for mildly to moderately active ulcerative colitis. A randomized study. N Engl J Med. 1987 Dec 24;317 (26):1625 - 9. doi: 10.1056/NEJM198712243172603.
- Rachmilewitz D. Coated mesalazine (5-aminosalicylic acid) versus sulphasalazine in the treatment of active ulcerative colitis: a randomised trial. BMJ. 1989 Jan 14;298 (6666):82 - 6.
- Голофеевский В. Ю., Герасимова А. В., Ситкин С. И., Асанин Ю. Ю. Индекс Масевича: новый подход к оценке клинико-эндоскопической активности язвенного колита // Гастроэнтерология Санкт-Петербурга. - 2004. - № 1. - С. 14 - 15.
- Орешко Л. С. Исторические и клинические аспекты целиакии. - СПб.: СПбГМА им. И. И. Мечникова, 2011. - 108 с.
- Парфенов А. И. Глютенчувствительная целиакия - мультидисциплинарная патология человека // Верхневолжский медицинский журнал. - 2013. - Т. 11, № 2. - С. 42 - 48.
- Лазебник Л. Б., Ткаченко Е. И., Орешко Л. С., Ситкин С. И., Карпов А. А., Немцов В. И., Осипенко М. Ф., Радченко В. Г., Федоров Е. Д., Медведева О. И., Селиверстов П. В., Соловьева Е. А., Шабанова А. А., Журавлева М. С. Рекомендации по диагностике и лечению целиакии взрослых // Экспериментальная и клиническая гастроэнтерология. - 2015. - № 5 (117). - С. 3 - 12.
- Penders J, Thijs C, van den Brandt PA, Kummeling I, Snijders B, Stelma F, Adams H, van Ree R, Stobberingh EE. Gut microbiota composition and development of atopic manifestations in infancy: the KOALA Birth Cohort Study. Gut. 2007 May; 56 (5):661 - 7. doi: 10.1136/gut. 2006.100164.
- Smith B, Li N, Andersen AS, Slotved HC, Krogfelt KA. Optimising bacterial DNA extraction from faecal samples: comparison of three methods. Open Microbiol J. 2011;5:14 - 7. doi: 10.2174/1874285801105010014.
- Liu C, Song Y, McTeague M, Vu AW, Wexler H, Finegold SM. Rapid identification of the species of the Bacteroides fragilis group by multiplex PCR assays using group- and species-specific primers. FEMS Microbiol Lett. 2003 May 16;222 (1):9 - 16.
- Rinttilä T., Kassinen A, Malinen E, Krogius L, Palva A. Development of an extensive set of 16S rDNA-targeted primers for quantification of pathogenic and indigenous bacteria in faecal samples by real-time PCR. J Appl Microbiol. 2004;97 (6):1166 - 77. doi: 10.1111/j. 1365 - 2672.2004.02409.x.
- Penders J, Thijs C, Vink C, Stelma FF, Snijders B, Kummeling I, van den Brandt PA, Stobberingh EE. Factors influencing the composition of the intestinal microbiota in early infancy. Pediatrics. 2006 Aug; 118 (2):511 - 21. doi: 10.1542/peds. 2005 - 2824.
- Sokol H, Seksik P, Furet JP, Firmesse O, Nion-Larmurier I, Beaugerie L, Cosnes J, Corthier G, Marteau P, Doré J. Low counts of Faecalibacterium prausnitzii in colitis microbiota. Inflamm Bowel Dis. 2009 Aug; 15 (8):1183 - 9. doi: 10.1002/ibd. 20903.
- Louis P, Flint HJ. Development of a semiquantitative degenerate real-time pcr-based assay for estimation of numbers of butyryl-coenzyme A (CoA) CoA transferase genes in complex bacterial samples. Appl Environ Microbiol. 2007 Mar; 73 (6):2009 - 12. doi: 10.1128/AEM. 02561 - 06.
- Louis P, Flint HJ. Diversity, metabolism and microbial ecology of butyrate-producing bacteria from the human large intestine. FEMS Microbiol Lett. 2009 May; 294 (1):1 - 8. doi: 10.1111/j. 1574 - 6968.2009.01514.x.
- Гржибовский А. М. Типы данных, проверка распределения и описательная статистика // Экология человека. - 2008. - № 1. - С. 52 - 58.
- Банержи A. Медицинская статистка понятным языком: вводный курс / пер. с англ. под ред. В. П. Леонова. - М.: Практическая медицина, 2014. - 287 с.
- Гублер Е. В., Генкин А. А. Применение непараметрических критериев статистики в медико-биологических исследованиях. - Л.: Медицина. - 1973. - 141 с.
- Гржибовский А. М. Анализ количественных данных для двух независимых групп // Экология человека. - 2008. - № 2. - С. 54 - 61.
- Наследов А. SPSS 19: профессиональный статистический анализ данных. - СПб.: Питер, 2011. - 400 с.
- Eckburg PB, Bik EM, Bernstein CN, Purdom E, Dethlefsen L, Sargent M, Gill SR, Nelson KE, Relman DA. Diversity of the human intestinal microbial flora. Science. 2005 Jun 10;308 (5728):1635 - 8. doi: 10.1126/science. 1110591.
- Hong PY, Wu JH, Liu WT. Relative abundance of Bacteroides spp. in stools and wastewaters as determined by hierarchical oligonucleotide primer extension. Appl Environ Microbiol. 2008 May; 74 (9):2882 - 93. doi: 10.1128/AEM. 02568 - 07.
- Sakamoto M, Benno Y. Reclassification of Bacteroides distasonis, Bacteroides goldsteinii and Bacteroides merdae as Parabacteroides distasonis gen. nov., comb. nov., Parabacteroides goldsteinii comb. nov. and Parabacteroides merdae comb. nov. Int J Syst Evol Microbiol. 2006 Jul; 56 (Pt 7):1599 - 605. doi: 10.1099/ijs. 0.64192 - 0.
- Nakanishi H, Shojo H, Ohmori T, Hara M, Takada A, Adachi N, Saito K. Identification of feces by detection of Bacteroides genes. Forensic Sci Int Genet. 2013 Jan; 7 (1):176 - 9. doi: 10.1016/j. fsigen. 2012.09.006.
- Kabiri L, Alum A, Rock C, McLain JE, Abbaszadegan M. Isolation of Bacteroides from fish and human fecal samples for identification of unique molecular markers. Can J Microbiol. 2013 Dec; 59 (12):771 - 7. doi: 10.1139/cjm-2013 - 0518.
- Ткаченко Е. И. Питание, эндоэкология человека, здоровье, болезни. Современный взгляд на проблему их взаимосвязей // Терапевтический архив. - 2004. - Т. 76, № 2. - С. 67 - 71.
- Вахитов Т. Я., Ситкин С. И. Концепция суперорганизма в биологии и медицине // Экспериментальная и клиническая гастроэнтерология. - 2014. - № 7 (107). - С. 72 - 85.
- Heinken A, Sahoo S, Fleming RM, Thiele I. Systems-level characterization of a host-microbe metabolic symbiosis in the mammalian gut. Gut Microbes. 2013 Jan-Feb; 4 (1):28 - 40. doi: 10.4161/gmic. 22370.
- Frank DN, St Amand AL, Feldman RA, Boedeker EC, Harpaz N, Pace NR. Molecular-phylogenetic characterization of microbial community imbalances in human inflammatory bowel diseases. Proc Natl Acad Sci U S A. 2007 Aug 21;104 (34):13780 - 5. doi: 10.1073/pnas. 0706625104.
- Troy EB, Kasper DL. Beneficial effects of Bacteroides fragilis polysaccharides on the immune system. Front Biosci (Landmark Ed). 2010 Jan 1;15:25 - 34.
- Hooper LV, Stappenbeck TS, Hong CV, Gordon JI. Angiogenins: a new class of microbicidal proteins involved in innate immunity. Nat Immunol. 2003 Mar; 4 (3):269 - 73. doi: 10.1038/ni888.
- Narimani T, Douraghi M, Owlia P, Rastegar A, Esghaei M, Nasr B, Talebi M. Heterogeneity in resistant fecal Bacteroides fragilis group collected from healthy people. Microb Pathog. 2016 Jun; 95:1 - 6. doi: 10.1016/j. micpath. 2016.02.017.
- Wexler HM. Bacteroides: the good, the bad, and the nitty-gritty. Clin Microbiol Rev. 2007 Oct; 20 (4):593 - 621. doi: 10.1128/CMR. 00008 - 07.
- Helphingstine CJ, Hentges DJ, Campbell BJ, Butt J, Barrett JT. Antibodies detectable by counterimmunoelectrophoresis against Bacteroides antigens in serum of patients with inflammatory bowel disease. J Clin Microbiol. 1979 Mar; 9 (3):373 - 8.
- Bamba T, Matsuda H, Endo M, Fujiyama Y. The pathogenic role of Bacteroides vulgatus in patients with ulcerative colitis. J Gastroenterol. 1995 Nov; 30 Suppl 8:45 - 7.
- Saitoh S, Noda S, Aiba Y, Takagi A, Sakamoto M, Benno Y, Koga Y. Bacteroides ovatus as the predominant commensal intestinal microbe causing a systemic antibody response in inflammatory bowel disease. Clin Diagn Lab Immunol. 2002 Jan; 9 (1):54 - 9.
- Iltanen S, Tervo L, Halttunen T, Wei B, Braun J, Rantala I, Honkanen T, Kronenberg M, Cheroutre H, Turovskaya O, Autio V, Ashorn M. Elevated serum anti-I2 and anti-OmpW antibody levels in children with IBD. Inflamm Bowel Dis. 2006 May; 12 (5):389 - 94. doi: 10.1097/01. MIB. 0000218765.84087.42.
- Frehn L, Jansen A, Bennek E, Mandic AD, Temizel I, Tischendorf S, Verdier J, Tacke F, Streetz K, Trautwein C, Sellge G. Distinct patterns of IgG and IgA against food and microbial antigens in serum and feces of patients with inflammatory bowel diseases. PLoS One. 2014 Sep 12;9 (9):e106750. doi: 10.1371/journal. pone. 0106750.
- Tvede M, Bondesen S, Nielsen OH, Rasmussen SN. Serum antibodies to Bacteroides species in chronic inflammatory bowel disease. Scand J Gastroenterol. 1983 Sep; 18 (6):783 - 9.
- Campieri M, Gionchetti P. Bacteria as the cause of ulcerative colitis. Gut. 2001 Jan; 48 (1):132 - 5.
- Ashorn S, Honkanen T, Kolho KL, Ashorn M, Välineva T, Wei B, Braun J, Rantala I, Luukkaala T, Iltanen S. Fecal calprotectin levels and serological responses to microbial antigens among children and adolescents with inflammatory bowel disease. Inflamm Bowel Dis. 2009 Feb; 15 (2):199 - 205. doi: 10.1002/ibd. 20535.
- Sydora BC, Tavernini MM, Doyle JS, Fedorak RN. Association with selected bacteria does not cause enterocolitis in IL-10 gene-deficient mice despite a systemic immune response. Dig Dis Sci. 2005 May; 50 (5):905 - 13.
- Swidsinski A, Weber J, Loening-Baucke V, Hale LP, Lochs H. Spatial organization and composition of the mucosal flora in patients with inflammatory bowel disease. J Clin Microbiol. 2005 Jul; 43 (7):3380 - 9. doi: 10.1128/JCM. 43.7.3380 - 3389.2005.
- Lucke K, Miehlke S, Jacobs E, Schuppler M. Prevalence of Bacteroides and Prevotella spp. in ulcerative colitis. J Med Microbiol. 2006 May; 55 (Pt 5):617 - 24. doi: 10.1099/jmm. 0.46198 - 0.
- Kabeerdoss J, Jayakanthan P, Pugazhendhi S, Ramakrishna BS. Alterations of mucosal microbiota in the colon of patients with inflammatory bowel disease revealed by real time polymerase chain reaction amplification of 16S ribosomal ribonucleic acid. Indian J Med Res. 2015 Jul; 142 (1):23 - 32. doi: 10.4103/0971 - 5916.162091.
- Zhang T, Chen Y, Wang Z, Zhou Y, Zhang S, Wang P, Xie S, Jiang B. [Changes of fecal flora and its correlation with inflammatory indicators in patients with inflammatory bowel disease]. [Article in Chinese] Nan Fang Yi Ke Da Xue Xue Bao. 2013 Oct; 33 (10):1474 - 7.
- Yao P, Cui M, Wang H, Gao H, Wang L, Yang T, Cheng Y. Quantitative Analysis of Intestinal Flora of Uygur and Han Ethnic Chinese Patients with Ulcerative Colitis. Gastroenterol Res Pract. 2016;2016:9186232. doi: 10.1155/2016/9186232.
- Jansson J, Willing B, Lucio M, Fekete A, Dicksved J, Halfvarson J, Tysk C, Schmitt-Kopplin P. Metabolomics reveals metabolic biomarkers of Crohn’s disease. PLoS One. 2009 Jul 28;4 (7):e6386. doi: 10.1371/journal. pone. 0006386.
- Conte MP, Schippa S, Zamboni I, Penta M, Chiarini F, Seganti L, Osborn J, Falconieri P, Borrelli O, Cucchiara S. Gut-associated bacterial microbiota in paediatric patients with inflammatory bowel disease. Gut. 2006 Dec; 55 (12):1760 - 7. doi: 10.1136/gut. 2005.078824.
- Fite A, Macfarlane S, Furrie E, Bahrami B, Cummings JH, Steinke DT, Macfarlane GT. Longitudinal analyses of gut mucosal microbiotas in ulcerative colitis in relation to patient age and disease severity and duration. J Clin Microbiol. 2013 Mar; 51 (3):849 - 56. doi: 10.1128/JCM. 02574 - 12.
- Takaishi H, Matsuki T, Nakazawa A, Takada T, Kado S, Asahara T, Kamada N, Sakuraba A, Yajima T, Higuchi H, Inoue N, Ogata H, Iwao Y, Nomoto K, Tanaka R, Hibi T. Imbalance in intestinal microflora constitution could be involved in the pathogenesis of inflammatory bowel disease. Int J Med Microbiol. 2008 Jul; 298 (5-6):463 - 72. doi: 10.1016/j. ijmm. 2007.07.016.
- Nemoto H, Kataoka K, Ishikawa H, Ikata K, Arimochi H, Iwasaki T, Ohnishi Y, Kuwahara T, Yasutomo K. Reduced diversity and imbalance of fecal microbiota in patients with ulcerative colitis. Dig Dis Sci. 2012 Nov; 57 (11):2955 - 64. doi: 10.1007/s10620-012-2236-y.
- Noor SO, Ridgway K, Scovell L, Kemsley EK, Lund EK, Jamieson C, Johnson IT, Narbad A. Ulcerative colitis and irritable bowel patients exhibit distinct abnormalities of the gut microbiota. BMC Gastroenterol. 2010 Nov 12;10:134. doi: 10.1186/1471-230X-10 - 134.
- Casén C, Vebø HC, Sekelja M, Hegge FT, Karlsson MK, Ciemniejewska E, Dzankovic S, Frøyland C, Nestestog R, Engstrand L, Munkholm P, Nielsen OH, Rogler G, Simrén M, Öhman L, Vatn MH, Rudi K. Deviations in human gut microbiota: a novel diagnostic test for determining dysbiosis in patients with IBS or IBD. Aliment Pharmacol Ther. 2015 Jul; 42 (1):71 - 83. doi: 10.1111/apt. 13236.
- Thorkildsen LT, Nwosu FC, Avershina E, Ricanek P, Perminow G, Brackmann S, Vatn MH, Rudi K. Dominant fecal microbiota in newly diagnosed untreated inflammatory bowel disease patients. Gastroenterol Res Pract. 2013;2013:636785. doi: 10.1155/2013/636785.
- Bloom SM, Bijanki VN, Nava GM, Sun L, Malvin NP, Donermeyer DL, Dunne WM Jr, Allen PM, Stappenbeck TS. Commensal Bacteroides species induce colitis in host-genotype-specific fashion in a mouse model of inflammatory bowel disease. Cell Host Microbe. 2011 May 19;9 (5):390 - 403. doi: 10.1016/j. chom. 2011.04.009.
- Ohkusa T, Yoshida T, Sato N, Watanabe S, Tajiri H, Okayasu I. Commensal bacteria can enter colonic epithelial cells and induce proinflammatory cytokine secretion: a possible pathogenic mechanism of ulcerative colitis. J Med Microbiol. 2009 May; 58 (Pt 5):535 - 45. doi: 10.1099/jmm. 0.005801 - 0.
- Sato K, Kumita W, Ode T, Ichinose S, Ando A, Fujiyama Y, Chida T, Okamura N. OmpA variants affecting the adherence of ulcerative colitis-derived Bacteroides vulgatus. J Med Dent Sci. 2010 Mar; 57 (1):55 - 64.
- Hickey CA, Kuhn KA, Donermeyer DL, Porter NT, Jin C, Cameron EA, Jung H, Kaiko GE, Wegorzewska M, Malvin NP, Glowacki RW, Hansson GC, Allen PM, Martens EC, Stappenbeck TS. Colitogenic Bacteroides thetaiotaomicron Antigens Access Host Immune Cells in a Sulfatase-Dependent Manner via Outer Membrane Vesicles. Cell Host Microbe. 2015 May 13;17 (5):672 - 80. doi: 10.1016/j. chom. 2015.04.002.
- Rhee KJ, Wu S, Wu X, Huso DL, Karim B, Franco AA, Rabizadeh S, Golub JE, Mathews LE, Shin J, Sartor RB, Golenbock D, Hamad AR, Gan CM, Housseau F, Sears CL. Induction of persistent colitis by a human commensal, enterotoxigenic Bacteroides fragilis, in wild-type C57BL/6 mice. Infect Immun. 2009 Apr; 77 (4):1708 - 18. doi: 10.1128/IAI. 00814 - 08.
- Mazmanian SK, Round JL, Kasper DL. A microbial symbiosis factor prevents intestinal inflammatory disease. Nature. 2008 May 29;453 (7195):620 - 5. doi: 10.1038/nature07008.
- Waidmann M, Bechtold O, Frick JS, Lehr HA, Schubert S, Dobrindt U, Loeffler J, Bohn E, Autenrieth IB. Bacteroides vulgatus protects against Escherichia coli-induced colitis in gnotobiotic interleukin-2-deficient mice. Gastroenterology. 2003 Jul; 125 (1):162 - 77.
- Hudcovic T, Kozáková H, Kolínská J, Stepánková R, Hrncír T, Tlaskalová-Hogenová H. Monocolonization with Bacteroides ovatus protects immunodeficient SCID mice from mortality in chronic intestinal inflammation caused by long-lasting dextran sodium sulfate treatment. Physiol Res. 2009;58 (1):101 - 10.
- Sánchez E, De Palma G, Capilla A, Nova E, Pozo T, Castillejo G, Varea V, Marcos A, Garrote JA, Polanco I, López A, Ribes-Koninckx C, García-Novo MD, Calvo C, Ortigosa L, Palau F, Sanz Y. Influence of environmental and genetic factors linked to celiac disease risk on infant gut colonization by Bacteroides species. Appl Environ Microbiol. 2011 Aug; 77 (15):5316 - 23. doi: 10.1128/AEM. 00365 - 11.
- Sánchez E, Laparra JM, Sanz Y. Discerning the role of Bacteroides fragilis in celiac disease pathogenesis. Appl Environ Microbiol. 2012 Sep; 78 (18):6507 - 15. doi: 10.1128/AEM. 00563 - 12.
- Hoffmann KM, Deutschmann A, Weitzer C, Joainig M, Zechner E, Högenauer C, Hauer AC. Antibiotic-associated hemorrhagic colitis caused by cytotoxin-producing Klebsiella oxytoca. Pediatrics. 2010 Apr; 125 (4):e960-3. doi: 10.1542/peds. 2009 - 1751.
- Ravcheev DA, Godzik A, Osterman AL, Rodionov DA. Polysaccharides utilization in human gut bacterium Bacteroides thetaiotaomicron: comparative genomics reconstruction of metabolic and regulatory networks. BMC Genomics. 2013 Dec 12;14:873. doi: 10.1186/1471-2164-14-873.
- Cantarel BL, Lombard V, Henrissat B. Complex carbohydrate utilization by the healthy human microbiome. PLoS One. 2012;7 (6):e28742. doi: 10.1371/journal. pone. 0028742.
- Xu J, Bjursell MK, Himrod J, Deng S, Carmichael LK, Chiang HC, Hooper LV, Gordon JI. A genomic view of the human-Bacteroides thetaiotaomicron symbiosis. Science. 2003 Mar 28;299 (5615):2074 - 6. doi: 10.1126/science. 1080029.
- Martens EC, Koropatkin NM, Smith TJ, Gordon JI. Complex glycan catabolism by the human gut microbiota: the Bacteroidetes Sus-like paradigm. J Biol Chem. 2009 Sep 11;284 (37):24673 - 7. doi: 10.1074/jbc. R109.022848.
- Martens EC, Lowe EC, Chiang H, Pudlo NA, Wu M, McNulty NP, Abbott DW, Henrissat B, Gilbert HJ, Bolam DN, Gordon JI. Recognition and degradation of plant cell wall polysaccharides by two human gut symbionts. PLoS Biol. 2011 Dec; 9 (12):e1001221. doi: 10.1371/journal. pbio. 1001221.
- Bolam DN, Koropatkin NM. Glycan recognition by the Bacteroidetes Sus-like systems. Curr Opin Struct Biol. 2012 Oct; 22 (5):563 - 9. doi: 10.1016/j. sbi. 2012.06.006.
- Koropatkin NM, Cameron EA, Martens EC. How glycan metabolism shapes the human gut microbiota. Nat Rev Microbiol. 2012 Apr 11;10 (5):323 - 35. doi: 10.1038/nrmicro2746.
- Ulmer JE, Vilén EM, Namburi RB, Benjdia A, Beneteau J, Malleron A, Bonnaffé D, Driguez PA, Descroix K, Lassalle G, Le Narvor C, Sandström C, Spillmann D, Berteau O. Characterization of glycosaminoglycan (GAG) sulfatases from the human gut symbiont Bacteroides thetaiotaomicron reveals the first GAG-specific bacterial endosulfatase. J Biol Chem. 2014 Aug 29;289 (35):24289 - 303. doi: 10.1074/jbc. M114.573303.
- Cameron EA, Kwiatkowski KJ, Lee BH, Hamaker BR, Koropatkin NM, Martens EC. Multifunctional nutrient-binding proteins adapt human symbiotic bacteria for glycan competition in the gut by separately promoting enhanced sensing and catalysis. MBio. 2014 Sep 9;5 (5):e01441-14. doi: 10.1128/mBio. 01441 - 14.
- Wrzosek L, Miquel S, Noordine ML, Bouet S, Joncquel Chevalier-Curt M, Robert V, Philippe C, Bridonneau C, Cherbuy C, Robbe-Masselot C, Langella P, Thomas M. Bacteroides thetaiotaomicron and Faecalibacterium prausnitzii influence the production of mucus glycans and the development of goblet cells in the colonic epithelium of a gnotobiotic model rodent. BMC Biol. 2013 May 21;11:61. doi: 10.1186/1741-7007-11-61.
- Woting A, Blaut M. The Intestinal Microbiota in Metabolic Disease. Nutrients. 2016 Apr 6;8 (4):202. doi: 10.3390/nu8040202.
- Kelly D, Campbell JI, King TP, Grant G, Jansson EA, Coutts AG, Pettersson S, Conway S. Commensal anaerobic gut bacteria attenuate inflammation by regulating nuclear-cytoplasmic shuttling of PPAR-gamma and RelA. Nat Immunol. 2004 Jan; 5 (1):104 - 12. doi: 10.1038/ni1018.
- Taketani M, Donia MS, Jacobson AN, Lambris JD, Fischbach MA. A Phase-Variable Surface Layer from the Gut Symbiont Bacteroides thetaiotaomicron. MBio. 2015 Sep 29;6 (5):e01339-15. doi: 10.1128/mBio. 01339 - 15.
- de Sablet T, Chassard C, Bernalier-Donadille A, Vareille M, Gobert AP, Martin C. Human microbiota-secreted factors inhibit shiga toxin synthesis by enterohemorrhagic Escherichia coli O157: H7. Infect Immun. 2009 Feb; 77 (2):783 - 90. doi: 10.1128/IAI. 01048 - 08.
- Cordonnier C, Le Bihan G, Emond-Rheault JG, Garrivier A, Harel J, Jubelin G. Vitamin B12 Uptake by the Gut Commensal Bacteria Bacteroides thetaiotaomicron Limits the Production of Shiga Toxin by Enterohemorrhagic Escherichia coli. Toxins (Basel). 2016 Jan 5;8 (1). pii: E14. doi: 10.3390/toxins8010014.
- Varyukhina S, Freitas M, Bardin S, Robillard E, Tavan E, Sapin C, Grill JP, Trugnan G. Glycan-modifying bacteria-derived soluble factors from Bacteroides thetaiotaomicron and Lactobacillus casei inhibit rotavirus infection in human intestinal cells. Microbes Infect. 2012 Mar; 14 (3):273 - 8. doi: 10.1016/j. micinf. 2011.10.007.
- Ferreyra JA, Wu KJ, Hryckowian AJ, Bouley DM, Weimer BC, Sonnenburg JL. Gut microbiota-produced succinate promotes C. difficile infection after antibiotic treatment or motility disturbance. Cell Host Microbe. 2014 Dec 10;16 (6):770 - 7. doi: 10.1016/j. chom. 2014.11.003.
- Curtis MM, Hu Z, Klimko C, Narayanan S, Deberardinis R, Sperandio V. The Gut Commensal Bacteroides thetaiotaomicron Exacerbates Enteric Infection through Modification of the Metabolic Landscape. Cell Host Microbe. 2014 Dec 10;16 (6):759 - 69. doi: 10.1016/j. chom. 2014.11.005.
- Iversen H, Lindbäck T, L’Abée-Lund TM, Roos N, Aspholm M, Stenfors Arnesen L. The gut bacterium Bacteroides thetaiotaomicron influences the virulence potential of the enterohemorrhagic Escherichia coli O103: H25. PLoS One. 2015 Feb 26;10 (2):e0118140. doi: 10.1371/journal. pone. 0118140.
- Macfarlane S, Macfarlane GT. Regulation of short-chain fatty acid production. Proc Nutr Soc. 2003 Feb; 62 (1):67 - 72. doi: 10.1079/PNS2002207.
- Mills E, O’Neill LA. Succinate: a metabolic signal in inflammation. Trends Cell Biol. 2014 May; 24 (5):313 - 20. doi: 10.1016/j. tcb. 2013.11.008.
- Wang A, Si H, Liu D, Jiang H. Butyrate activates the cAMP-protein kinase A-cAMP response element-binding protein signaling pathway in Caco-2 cells. J Nutr. 2012 Jan; 142 (1):1 - 6. doi: 10.3945/jn. 111.148155.
- Diakos C, Prieschl EE, Säemann M, Novotny V, Böhmig G, Csonga R, Baumruker T, Zlabinger GJ. Novel mode of interference with nuclear factor of activated T-cells regulation in T-cells by the bacterial metabolite n-butyrate. J Biol Chem. 2002 Jul 5;277 (27):24243 - 51. doi: 10.1074/jbc. M200191200
- Diakos C, Prieschl EE, Säemann MD, Böhmig GA, Csonga R, Sobanov Y, Baumruker T, Zlabinger GJ. n-Butyrate inhibits Jun NH (2) - terminal kinase activation and cytokine transcription in mast cells. Biochem Biophys Res Commun. 2006 Oct 20;349 (2):863 - 8. doi: 10.1016/j. bbrc. 2006.08.117
- Campbell Y, Fantacone ML, Gombart AF. Regulation of antimicrobial peptide gene expression by nutrients and by-products of microbial metabolism. Eur J Nutr. 2012 Dec; 51 (8):899 - 907. doi: 10.1007/s00394-012-0415-4.
- Arpaia N, Campbell C, Fan X, Dikiy S, van der Veeken J, deRoos P, Liu H, Cross JR, Pfeffer K, Coffer PJ, Rudensky AY. Metabolites produced by commensal bacteria promote peripheral regulatory T-cell generation. Nature. 2013 Dec 19;504 (7480):451 - 5. doi: 10.1038/nature12726.
- Furusawa Y, Obata Y, Fukuda S, Endo TA, Nakato G, Takahashi D, Nakanishi Y, Uetake C, Kato K, Kato T, Takahashi M, Fukuda NN, Murakami S, Miyauchi E, Hino S, Atarashi K, Onawa S, Fujimura Y, Lockett T Clarke JM, Topping DL, Tomita M, Hori S, Ohara O, Morita T, Koseki H, Kikuchi J, Honda K, Hase K, Ohno H. Commensal microbe-derived butyrate induces the differentiation of colonic regulatory T cells. Nature. 2013 Dec 19;504 (7480):446 - 50. doi: 10.1038/nature12721.
- Chang PV, Hao L, Offermanns S, Medzhitov R. The microbial metabolite butyrate regulates intestinal macrophage function via histone deacetylase inhibition. Proc Natl Acad Sci U S A. 2014 Feb 11;111 (6):2247 - 52. doi: 10.1073/pnas. 1322269111.
- Tamura K, Yamamura M, Satomi M. Effect of butyrate on colonic mucosa. JJPEN: Japanese Journal of Parenteral and Enteral Nutrition. 1995 17:481 - 4.
- Segain JP, Raingeard de la Blétière D, Bourreille A, Leray V, Gervois N, Rosales C, Ferrier L, Bonnet C, Blottière HM, Galmiche JP. Butyrate inhibits inflammatory responses through NFκB inhibition: implications for Crohn’s disease. Gut. 2000 Sep; 47 (3):397 - 403.
- Peng L, Li ZR, Green RS, Holzman IR, Lin J. Butyrate enhances the intestinal barrier by facilitating tight junction assembly via activation of AMP-activated protein kinase in Caco-2 cell monolayers. J Nutr. 2009 Sep; 139 (9):1619 - 25. doi: 10.3945/jn. 109.104638.
- Vinolo MA, Rodrigues HG, Hatanaka E, Sato FT, Sampaio SC, Curi R. Suppressive effect of short-chain fatty acids on production of proinflammatory mediators by neutrophils. J Nutr Biochem. 2011 Sep; 22 (9):849 - 55. doi: 10.1016/j. jnutbio. 2010.07.009.
- Lührs H, Kudlich T, Neumann M, Schauber J, Melcher R, Gostner A, Scheppach W, Menzel TP. Butyrate-enhanced TNFα-induced apoptosis is associated with inhibition of NF-κB. Anticancer Res. 2002 May-Jun; 22 (3):1561 - 8.
- Scharlau D, Borowicki A, Habermann N, Hofmann T, Klenow S, Miene C, Munjal U, Stein K, Glei M. Mechanisms of primary cancer prevention by butyrate and other products formed during gut flora-mediated fermentation of dietary fibre. Mutat Res. 2009 Jul-Aug; 682 (1):39 - 53. doi: 10.1016/j. mrrev. 2009.04.001.
- Lazarova DL, Chiaro C, Bordonaro M. Butyrate induced changes in Wnt-signaling specific gene expression in colorectal cancer cells. BMC Res Notes. 2014 Apr 9;7:226. doi: 10.1186/1756-0500-7-226.
- Pryde SE, Duncan SH, Hold GL, Stewart CS, Flint HJ. The microbiology of butyrate formation in the human colon. FEMS Microbiol Lett. 2002 Dec 17;217 (2):133 - 9.
- Barcenilla A, Pryde SE, Martin JC, Duncan SH, Stewart CS, Henderson C, Flint HJ. Phylogenetic relationships of butyrate-producing bacteria from the human gut. Appl Environ Microbiol. 2000 Apr; 66 (4):1654 - 61.
- Duncan SH, Barcenilla A, Stewart CS, Pryde SE, Flint HJ. Acetate utilization and butyryl coenzyme A (CoA):acetate-CoA transferase in butyrate-producing bacteria from the human large intestine. Appl Environ Microbiol. 2002 Oct; 68 (10):5186 - 90.
- Louis P, Young P, Holtrop G, Flint HJ. Diversity of human colonic butyrate-producing bacteria revealed by analysis of the butyryl-CoA: acetate CoA-transferase gene. Environ Microbiol. 2010 Feb; 12 (2):304 - 14. doi: 10.1111/j. 1462 - 2920.2009.02066.x.
- Vital M, Penton CR, Wang Q, Young VB, Antonopoulos DA, Sogin ML, Morrison HG, Raffals L, Chang EB, Huffnagle GB, Schmidt TM, Cole JR, Tiedje JM. A gene-targeted approach to investigate the intestinal butyrate-producing bacterial community. Microbiome. 2013 Mar 4;1 (1):8. doi: 10.1186/2049-2618-1-8.
- Bui TP, de Vos WM, Plugge CM. Anaerostipes rhamnosivorans sp. nov., a human intestinal, butyrate-forming bacterium. Int J Syst Evol Microbiol. 2014 Mar; 64 (Pt 3):787 - 93. doi: 10.1099/ijs. 0.055061 - 0.
- Vital M, Howe AC, Tiedje JM. Revealing the bacterial butyrate synthesis pathways by analyzing (meta) genomic data. MBio. 2014 Apr 22;5 (2):e00889. doi: 10.1128/mBio. 00889 - 14.
- Varela E, Manichanh C, Gallart M, Torrejón A, Borruel N, Casellas F, Guarner F, Antolin M. Colonisation by Faecalibacterium prausnitzii and maintenance of clinical remission in patients with ulcerative colitis. Aliment Pharmacol Ther. 2013 Jul; 38 (2):151 - 61. doi: 10.1111/apt. 12365.
- Wang W, Chen L, Zhou R, Wang X, Song L, Huang S, Wang G, Xia B. Increased proportions of Bifidobacterium and the Lactobacillus group and loss of butyrate-producing bacteria in inflammatory bowel disease. J Clin Microbiol. 2014 Feb; 52 (2):398 - 406. doi: 10.1128/JCM. 01500 - 13.
- Machiels K, Joossens M, Sabino J, De Preter V, Arijs I, Eeckhaut V, Ballet V, Claes K, Van Immerseel F, Verbeke K, Ferrante M, Verhaegen J, Rutgeerts P, Vermeire S. A decrease of the butyrate-producing species Roseburia hominis and Faecalibacterium prausnitzii defines dysbiosis in patients with ulcerative colitis. Gut. 2014 Aug; 63 (8):1275 - 83. doi: 10.1136/gutjnl-2013 - 304833.
- Cao Y, Shen J, Ran ZH. Association between Faecalibacterium prausnitzii Reduction and Inflammatory Bowel Disease: A Meta-Analysis and Systematic Review of the Literature. Gastroenterol Res Pract. 2014;2014:872725. doi: 10.1155/2014/872725.
- Zhang M, Liu B, Zhang Y, Wei H, Lei Y, Zhao L. Structural shifts of mucosa-associated lactobacilli and Clostridium leptum subgroup in patients with ulcerative colitis. J Clin Microbiol. 2007 Feb; 45 (2):496 - 500. doi: 10.1128/JCM. 01720 - 06.
- Vermeiren J, Van den Abbeele P, Laukens D, Vigsnaes LK, De Vos M, Boon N, Van de Wiele T. Decreased colonization of fecal Clostridium coccoides/Eubacterium rectale species from ulcerative colitis patients in an in vitro dynamic gut model with mucin environment. FEMS Microbiol Ecol. 2012 Mar; 79 (3):685 - 96. doi: 10.1111/j. 1574 - 6941.2011.01252.x.
- Morgan XC, Tickle TL, Sokol H, Gevers D, Devaney KL, Ward DV, Reyes JA, Shah SA, LeLeiko N, Snapper SB, Bousvaros A, Korzenik J, Sands BE, Xavier RJ, Huttenhower C. Dysfunction of the intestinal microbiome in inflammatory bowel disease and treatment. Genome Biol. 2012 Apr 16;13 (9):R79. doi: 10.1186/gb-2012-13-9-r79.
- Eeckhaut V, Machiels K, Perrier C, Romero C, Maes S, Flahou B, Steppe M, Haesebrouck F, Sas B, Ducatelle R, Vermeire S, Van Immerseel F. Butyricicoccus pullicaecorum in inflammatory bowel disease. Gut. 2013 Dec; 62 (12):1745 - 52. doi: 10.1136/gutjnl-2012 - 303611.
- Kumari R, Ahuja V, Paul J. Fluctuations in butyrate-producing bacteria in ulcerative colitis patients of North India. World J Gastroenterol. 2013 Jun 14;19 (22):3404 - 14. doi: 10.3748/wjg. v19.i22.3404.
- Chen L, Wang W, Zhou R, Ng SC, Li J, Huang M, Zhou F, Wang X, Shen B, A Kamm M, Wu K, Xia B. Characteristics of fecal and mucosa-associated microbiota in chinese patients with inflammatory bowel disease. Medicine (Baltimore). 2014 Aug; 93 (8):e51. doi: 10.1097/MD. 0000000000000051.
- Devriese S, Eeckhaut V, Geirnaert A, Van den Bossche L, Hindryckx P, Van de Wiele T, Van Immerseel F, Ducatelle R, De Vos M, Laukens D. Reduced mucosa-associated Butyricicoccus activity in patients with ulcerative colitis correlates with aberrant claudin-1 expression. J Crohns Colitis. 2016 Aug 1. pii: jjw142. doi: 10.1093/ecco-jcc/jjw142.
- Mahowald MA, Rey FE, Seedorf H, Turnbaugh PJ, Fulton RS, Wollam A, Shah N, Wang C, Magrini V, Wilson RK, Cantarel BL, Coutinho PM, Henrissat B, Crock LW, Russell A, Verberkmoes NC, Hettich RL, Gordon JI. Characterizing a model human gut microbiota composed of members of its two dominant bacterial phyla. Proc Natl Acad Sci U S A. 2009 Apr 7;106 (14):5859 - 64. doi: 10.1073/pnas. 0901529106.
- Png CW, Lindén SK, Gilshenan KS, Zoetendal EG, McSweeney CS, Sly LI, McGuckin MA, Florin TH. Mucolytic bacteria with increased prevalence in IBD mucosa augment in vitro utilization of mucin by other bacteria. Am J Gastroenterol. 2010 Nov; 105 (11):2420 - 8. doi: 10.1038/ajg. 2010.281.
- Vigsnæs LK, Brynskov J, Steenholdt C, Wilcks A, Licht TR. Gram-negative bacteria account for main differences between faecal microbiota from patients with ulcerative colitis and healthy controls. Benef Microbes. 2012 Dec 1;3 (4):287 - 97. doi: 10.3920/BM2012.0018.
- König J, Brummer RJ. Alteration of the intestinal microbiota as a cause of and a potential therapeutic option in irritable bowel syndrome. Benef Microbes. 2014 Sep; 5 (3):247 - 61. doi: 10.3920/BM2013.0033.
- Wang T, Cai G, Qiu Y, Fei N, Zhang M, Pang X, Jia W, Cai S, Zhao L. Structural segregation of gut microbiota between colorectal cancer patients and healthy volunteers. ISME J. 2012 Feb; 6 (2):320 - 9. doi: 10.1038/ismej. 2011.109.
- Weir TL, Manter DK, Sheflin AM, Barnett BA, Heuberger AL, Ryan EP. Stool microbiome and metabolome differences between colorectal cancer patients and healthy adults. PLoS One. 2013 Aug 6;8 (8):e70803. doi: 10.1371/journal. pone. 0070803.
- De Palma G, Nadal I, Medina M, Donat E, Ribes-Koninckx C, Calabuig M, Sanz Y. Intestinal dysbiosis and reduced immunoglobulin-coated bacteria associated with coeliac disease in children. BMC Microbiol. 2010 Feb 24;10:63. doi: 10.1186/1471-2180-10-63.
- Абдурасулова И. Н., Тарасова Е. А., Ермоленко Е. И., Елисеев А. В., Мацулевич А. В., Бисага Г. Н., Скулябин Д. И., Суворов А. Н., Клименко В. М. При рассеянном склерозе изменяется качественный и количественный состав микробиоты кишечника // Медицинский академический журнал. - 2015. - Том 15, № 3. - С. 55 - 67.
- Munukka E, Pekkala S, Wiklund P, Rasool O, Borra R, Kong L, Ojanen X, Cheng SM, Roos C, Tuomela S, Alen M, Lahesmaa R, Cheng S. Gut-adipose tissue axis in hepatic fat accumulation in humans. J Hepatol. 2014 Jul; 61 (1):132 - 8. doi: 10.1016/j. jhep. 2014.02.020.
- Chung WS, Walker AW, Louis P, Parkhill J, Vermeiren J, Bosscher D, Duncan SH, Flint HJ. Modulation of the human gut microbiota by dietary fibres occurs at the species level. BMC Biol. 2016 Jan 11;14:3. doi: 10.1186/s12915-015-0224-3.
- Kettle H, Donnelly R, Flint HJ, Marion G. pH feedback and phenotypic diversity within bacterial functional groups of the human gut. J Theor Biol. 2014 Feb 7;342:62 - 9. doi: 10.1016/j. jtbi. 2013.10.015.
- Shin R, Suzuki M, Morishita Y. Influence of intestinal anaerobes and organic acids on the growth of enterohaemorrhagic Escherichia coli O157: H7. J Med Microbiol. 2002 Mar; 51 (3):201 - 6. doi: 10.1099/0022-1317-51-3-201.
- Kamada N, Chen GY, Inohara N, Núñez G. Control of pathogens and pathobionts by the gut microbiota. Nat Immunol. 2013 Jul; 14 (7):685 - 90. doi: 10.1038/ni. 2608.
- Walker AW, Duncan SH, McWilliam Leitch EC, Child MW, Flint HJ. pH and peptide supply can radically alter bacterial populations and short-chain fatty acid ratios within microbial communities from the human colon. Appl Environ Microbiol. 2005 Jul; 71 (7):3692 - 700. doi: 10.1128/AEM. 71.7.3692 - 3700.2005.
- Duncan SH, Louis P, Thomson JM, Flint HJ. The role of pH in determining the species composition of the human colonic microbiota. Environ Microbiol. 2009 Aug; 11 (8):2112 - 22. doi: 10.1111/j. 1462 - 2920.2009.01931.x.
- Boesmans L, Ramakers M, Arijs I, Windey K, Vanhove W, Schuit F, Rutgeerts P, Verbeke K, De Preter V. Inflammation-Induced Downregulation of Butyrate Uptake and Oxidation Is Not Caused by a Reduced Gene Expression. J Cell Physiol. 2015 Feb; 230 (2):418 - 26. doi: 10.1002/jcp. 24725.
- DeMeo MT, Mutlu EA, Keshavarzian A, Tobin MC. Intestinal permeation and gastrointestinal disease. J Clin Gastroenterol. 2002 Apr; 34 (4):385 - 96.
- Thibault R, Blachier F, Darcy-Vrillon B, de Coppet P, Bourreille A, Segain JP. Butyrate utilization by the colonic mucosa in inflammatory bowel diseases: a transport deficiency. Inflamm Bowel Dis. 2010 Apr; 16 (4):684 - 95. doi: 10.1002/ibd. 21108.
- Kumar A, Alrefai WA, Borthakur A, Dudeja PK. Lactobacillus acidophilus counteracts enteropathogenic E. coli-induced inhibition of butyrate uptake in intestinal epithelial cells. Am J Physiol Gastrointest Liver Physiol. 2015 Oct 1;309 (7):G602-7. doi: 10.1152/ajpgi. 00186.2015.
- Hulin SJ, Singh S, Chapman MA, Allan A, Langman MJ, Eggo MC. Sulphide-induced energy deficiency in colonic cells is prevented by glucose but not by butyrate. Aliment Pharmacol Ther. 2002 Feb; 16 (2):325 - 31.
- Bullock NR, Booth JC, Gibson GR. Comparative composition of bacteria in the human intestinal microflora during remission and active ulcerative colitis. Curr Issues Intest Microbiol. 2004 Sep; 5 (2):59 - 64.
- Vigsnaes LK, van den Abbeele P, Sulek K, Frandsen HL, Steenholdt C, Brynskov J, Vermeiren J, van de Wiele T, Licht TR. Microbiotas from UC patients display altered metabolism and reduced ability of LAB to colonize mucus. Sci Rep. 2013;3:1110. doi: 10.1038/srep01110.
- Fyderek K, Strus M, Kowalska-Duplaga K, Gosiewski T, Wedrychowicz A, Jedynak-Wasowicz U, Sładek M, Pieczarkowski S, Adamski P, Kochan P, Heczko PB. Mucosal bacterial microflora and mucus layer thickness in adolescents with inflammatory bowel disease. World J Gastroenterol. 2009 Nov 14;15 (42):5287 - 94.
- Giaffer MH, Holdsworth CD, Duerden BI. The assessment of faecal flora in patients with inflammatory bowel disease by a simplified bacteriological technique. J Med Microbiol. 1991 Oct; 35 (4):238 - 43. doi: 10.1099/00222615-35-4-238.
- Mylonaki M, Rayment NB, Rampton DS, Hudspith BN, Brostoff J. Molecular characterization of rectal mucosa-associated bacterial flora in inflammatory bowel disease. Inflamm Bowel Dis. 2005 May; 11 (5):481 - 7.
- Goh YJ, Klaenhammer TR. Genomic features of Lactobacillus species. Front Biosci (Landmark Ed). 2009 Jan 1;14:1362 - 86.
- Mikelsaar M, Sepp E, Štšepetova J, Songisepp E, Mändar R. Biodiversity of Intestinal Lactic Acid Bacteria in the Healthy Population. Adv Exp Med Biol. 2016;932:1 - 64. doi: 10.1007/5584_2016_3.
- von Schillde MA, Hörmannsperger G, Weiher M, Alpert CA, Hahne H, Bäuerl C, van Huynegem K, Steidler L, Hrncir T, Pérez-Martínez G, Kuster B, Haller D. Lactocepin secreted by Lactobacillus exerts anti-inflammatory effects by selectively degrading proinflammatory chemokines. Cell Host Microbe. 2012 Apr 19;11 (4):387 - 96. doi: 10.1016/j. chom. 2012.02.006.
- Al-Hassi HO, Mann ER, Sanchez B, English NR, Peake ST, Landy J, Man R, Urdaci M, Hart AL, Fernandez-Salazar L, Lee GH, Garrote JA, Arranz E, Margolles A, Stagg AJ, Knight SC, Bernardo D. Altered human gut dendritic cell properties in ulcerative colitis are reversed by Lactobacillus plantarum extracellular encrypted peptide STp. Mol Nutr Food Res. 2014 May; 58 (5):1132 - 43. doi: 10.1002/mnfr. 201300596.
- Tsilingiri K, Barbosa T, Penna G, Caprioli F, Sonzogni A, Viale G, Rescigno M. Probiotic and postbiotic activity in health and disease: comparison on a novel polarised ex-vivo organ culture model. Gut. 2012 Jul; 61 (7):1007 - 15. doi: 10.1136/gutjnl-2011 - 300971.
- Farina C, Arosio M, Mangia M, Moioli F. Lactobacillus casei subsp. rhamnosus sepsis in a patient with ulcerative colitis. J Clin Gastroenterol. 2001 Sep; 33 (3):251 - 2.
- Vahabnezhad E, Mochon AB, Wozniak LJ, Ziring DA. Lactobacillus bacteremia associated with probiotic use in a pediatric patient with ulcerative colitis. J Clin Gastroenterol. 2013 May-Jun; 47 (5):437 - 9. doi: 10.1097/MCG. 0b013e318279abf0.
- Meini S, Laureano R, Fani L, Tascini C, Galano A, Antonelli A, Rossolini GM. Breakthrough Lactobacillus rhamnosus GG bacteremia associated with probiotic use in an adult patient with severe active ulcerative colitis: case report and review of the literature. Infection. 2015 Dec; 43 (6):777 - 81. doi: 10.1007/s15010-015-0798-2.
- Sheikhi A, Shakerian M, Giti H, Baghaeifar M, Jafarzadeh A, Ghaed V, Heibor MR, Baharifar N, Dadafarin Z, Bashirpour G. Probiotic Yogurt Culture Bifidobacterium Animalis Subsp. Lactis BB-12 and Lactobacillus Acidophilus LA-5 Modulate the Cytokine Secretion by Peripheral Blood Mononuclear Cells from Patients with Ulcerative Colitis. Drug Res (Stuttg). 2016 Jun; 66 (6):300 - 5. doi: 10.1055/s-0035 - 1569414.
- Guarner F, Khan AG, Garisch J, Eliakim R, Gangl A, Thomson A, Krabshuis J, Lemair T, Kaufmann P, de Paula JA, Fedorak R, Shanahan F, Sanders ME, Szajewska H, Ramakrishna BS, Karakan T, Kim N; World Gastroenterology Organization. World Gastroenterology Organisation Global Guidelines: probiotics and prebiotics October 2011. J Clin Gastroenterol. 2012 Jul; 46 (6):468 - 81. doi: 10.1097/MCG. 0b013e3182549092.
- Mardini HE, Grigorian AY. Probiotic mix VSL#3 is effective adjunctive therapy for mild to moderately active ulcerative colitis: a meta-analysis. Inflamm Bowel Dis. 2014 Sep; 20 (9):1562 - 7. doi: 10.1097/MIB. 0000000000000084.
- Floch MH, Walker WA, Sanders ME, Nieuwdorp M, Kim AS, Brenner DA, Qamar AA, Miloh TA, Guarino A, Guslandi M, Dieleman LA, Ringel Y, Quigley EM, Brandt LJ. Recommendations for Probiotic Use - 2015 Update: Proceedings and Consensus Opinion. J Clin Gastroenterol. 2015 Nov-Dec; 49 Suppl 1: S69-73. doi: 10.1097/MCG. 0000000000000420.
- Zocco MA, dal Verme LZ, Cremonini F, Piscaglia AC, Nista EC, Candelli M, Novi M, Rigante D, Cazzato IA, Ojetti V, Armuzzi A, Gasbarrini G, Gasbarrini A. Efficacy of Lactobacillus GG in maintaining remission of ulcerative colitis. Aliment Pharmacol Ther. 2006 Jun 1;23 (11):1567 - 74. doi: 10.1111/j. 1365 - 2036.2006.02927.x.
- Adams SM, Bornemann PH. Ulcerative colitis. Am Fam Physician. 2013 May 15;87 (10):699 - 705.
- Macfarlane S, Furrie E, Kennedy A, Cummings JH, Macfarlane GT. Mucosal bacteria in ulcerative colitis. Br J Nutr. 2005 Apr; 93 Suppl 1: S67-72.
- Орлова Н. А., Ситкин С. И., Ткаченко Е. И. Сравнительная оценка динамики показателей кишечной микрофлоры у больных воспалительными заболеваниями кишечника на фоне применения пробиотиков «Биофанк» и «Бифиформ» // Гастроэнтерология Санкт-Петербурга. - 2006. - № 1 - 2. - С. М113.
- Maukonen J, Kolho KL, Paasela M, Honkanen J, Klemetti P, Vaarala O, Saarela M. Altered fecal microbiota in pediatric inflammatory bowel disease. J Crohns Colitis. 2015 Dec; 9 (12):1088 - 95. doi: 10.1093/ecco-jcc/jjv147.
- Moran JP, Walter J, Tannock GW, Tonkonogy SL, Sartor RB. Bifidobacterium animalis causes extensive duodenitis and mild colonic inflammation in monoassociated interleukin-10-deficient mice. Inflamm Bowel Dis. 2009 Jul; 15 (7):1022 - 31. doi: 10.1002/ibd. 20900.
- Elian SD, Souza EL, Vieira AT, Teixeira MM, Arantes RM, Nicoli JR, Martins FS. Bifidobacterium longum subsp. infantis BB-02 attenuates acute murine experimental model of inflammatory bowel disease. Benef Microbes. 2015;6 (3):277 - 86. doi: 10.3920/BM2014.0070.
- Konieczna P, Akdis CA, Quigley EM, Shanahan F, O’Mahony L. Portrait of an immunoregulatory Bifidobacterium. Gut Microbes. 2012 May-Jun; 3 (3):261 - 6. doi: 10.4161/gmic. 20358.
- Groeger D, O’Mahony L, Murphy EF, Bourke JF, Dinan TG, Kiely B, Shanahan F, Quigley EM. Bifidobacterium infantis 35624 modulates host inflammatory processes beyond the gut. Gut Microbes. 2013 Jul-Aug; 4 (4):325 - 39. doi: 10.4161/gmic. 25487.
- Wildt S, Nordgaard I, Hansen U, Brockmann E, Rumessen JJ. A randomised double-blind placebo-controlled trial with Lactobacillus acidophilus La-5 and Bifidobacterium animalis subsp. lactis BB-12 for maintenance of remission in ulcerative colitis. J Crohns Colitis. 2011 Apr; 5 (2):115 - 21. doi: 10.1016/j. crohns. 2010.11.004.
- Tamaki H, Nakase H, Inoue S, Kawanami C, Itani T, Ohana M, Kusaka T, Uose S, Hisatsune H, Tojo M, Noda T, Arasawa S, Izuta M, Kubo A, Ogawa C, Matsunaka T, Shibatouge M. Efficacy of probiotic treatment with Bifidobacterium longum 536 for induction of remission in active ulcerative colitis: A randomized, double-blinded, placebo-controlled multicenter trial. Dig Endosc. 2016 Jan; 28 (1):67 - 74. doi: 10.1111/den. 12553.
- Weber E, Reynaud Q, Suy F, Gagneux-Brunon A, Carricajo A, Guillot A, Botelho-Nevers E. Bifidobacterium species bacteremia: risk factors in adults and infants. Clin Infect Dis. 2015 Aug 1;61 (3):482 - 4. doi: 10.1093/cid/civ347.
- Sanz Y, Sánchez E, Marzotto M, Calabuig M, Torriani S, Dellaglio F. Differences in faecal bacterial communities in coeliac and healthy children as detected by PCR and denaturing gradient gel electrophoresis. FEMS Immunol Med Microbiol. 2007 Dec; 51 (3):562 - 8. doi: 10.1111/j. 1574-695X. 2007.00337.x.
- Collado MC, Donat E, Ribes-Koninckx C, Calabuig M, Sanz Y. Imbalances in faecal and duodenal Bifidobacterium species composition in active and non-active coeliac disease. BMC Microbiol. 2008 Dec 22;8:232. doi: 10.1186/1471-2180-8-232.
- Nistal E, Caminero A, Vivas S, Ruiz de Morales JM, Sáenz de Miera LE, Rodríguez-Aparicio LB, Casqueiro J. Differences in faecal bacteria populations and faecal bacteria metabolism in healthy adults and celiac disease patients. Biochimie. 2012 Aug; 94 (8):1724 - 9. doi: 10.1016/j. biochi. 2012.03.025.
- Smecuol E, Hwang HJ, Sugai E, Corso L, Cherñavsky AC, Bellavite FP, González A, Vodánovich F, Moreno ML, Vázquez H, Lozano G, Niveloni S, Mazure R, Meddings J, Mauriño E, Bai JC. Exploratory, randomized, double-blind, placebo-controlled study on the effects of Bifidobacterium infantis natren life start strain super strain in active celiac disease. J Clin Gastroenterol. 2013 Feb; 47 (2):139 - 47. doi: 10.1097/MCG. 0b013e31827759ac.
- Sitkin S., Tkachenko E., Vakhitov T., Oreshko L., Zhigalova T. Oral butyrate plus inulin improve serum metabolomic profile and gut microbiota composition in ulcerative colitis and celiac disease. J Crohns Colitis. 2014;8 (Suppl 1):S232. doi: 10.1016/S1873-9946 (14) 60519 - 5.
- Shenderov BA. Metabiotics: novel idea or natural development of probiotic conception. Microb Ecol Health Dis. 2013 Apr 12;24. doi: 10.3402/mehd. v24i0.20399.
- Rios-Covian D, Gueimonde M, Duncan SH, Flint HJ, de Los Reyes-Gavilan CG. Enhanced butyrate formation by cross-feeding between Faecalibacterium prausnitzii and Bifidobacterium adolescentis. FEMS Microbiol Lett. 2015 Nov; 362 (21). pii: fnv176. doi: 10.1093/femsle/fnv176.
Опубликовано :
МИКРОБИОТА КИШЕЧНИКА ПРИ ЯЗВЕННОМ КОЛИТЕ И ЦЕЛИАКИИ. Экспериментальная и клиническая гастроэнтерология. 2017;137(01):08-30
Загрузить полный текст
-
- Ташкентский Педиатрический Медицинский Институт (Ташкент, Узбекистан)
Ключевые слова:дети,микроэлементы,макроэлементы
Резюме:Проведены исследования c целью оценки влияния на рост и развитие новорожденных уровня содержания некоторых микроэлементов, и особенностей взаимосвязи различных групп микроэлементов в организме детей. Изложены наиболее частые причины дефицита и избытка макро- и микроэлементов, выделены группы риска по развитию микроэлементозов. Дефицит биоэлементов является частой причиной серьезных нарушений функционирования органов и систем, внутриутробной задержки развития плода, анемии, что приводит к рождению детей с малым весом и увеличению заболеваемости в неонатальном периоде.
-
- Абатуров А. Е. Микроэлементный баланс и противоинфекционная защита у детей // Здоровье ребенка. - 2008. - № 1 (10). - С. 47 - 50.
- Башкірова Л., Руденко А. Біологічна роль деяких есенційних макро- та мікроелементів (огляд) // Ліки України. - 2004. - № 10. - С. 59 - 65.
- Бут Г. Микроэлементы и их роль в обеспечении иммунного ответа // Новости медицины и фармации. - 2008. - № 4 (235). - С. 13.
- Громова О. А. Школа по витаминам и микроэлементам. - М., 2004. - 59 с.
- Кудрин А. В., Скальный А. В., Жаворонков А. А. и др. Иммунофармакология микроэлементов. - М.: Изд-во КМК, 2000. - 537 с.
- Коровина Н. А., Захарова И. Н., Заплатников А. Л. Профилактика дефицита витаминов и микроэлементов у детей: Справочное пособие для врачей. - М., 2000. - 74 с.
- Нарушения минерального обмена у человека: Методическое пособие для врачей. - Донецк, 2006. - 82 с.
- Пшендин П. И. Рациональное питание спортсменов. - Олимп, 2003 - 114 с.
- Радучич О. Азбука здоровья // Здоров’я України. - 2007. - № 5. - С. 57.
- Роль микро- и макроэлементов в жизнедеятельности организма // Medicus Amicus, 2004. - № 4. - С. 18 - 23.
- Серебровская Н. Микроэлементы и здоровье // Нубель Эcтeтик, 2004. - № 6. - С. 11 - 16.
- Brown J. M., Pfau J. C., Holian A. Immunoglobulin and lymphocyte responses following silica exposure in New Zealand mixed mice // Inhal. Toxicol. - 2004. - Vol. 16, № 3. - P. 133 - 139.
- Failla M. Trace Elements and Host Defense: Recent Advances and Continuing Challenges // J. Nutr. - 2003. - Vol. 133. - P. 1443S-1447S.
- Benes B., Sladka J., Spevackova V. et al. Determination of normal concentration levels of Cd, Cr, Cu, Hg, Pb, Se and Zn in hair of the child population in the Czech Republic // Centr. Eur. J. Public Health. - 2003. - Vol. 11, № 4. - P. 184 - 186.
- Cavill I., Auerbach M., Bailie G. R. et al. Iron and the anaemia of chronic disease: a review and strategic recommendations // Curr. Med. Res. Opin. - 2006. - Vol. 22, № 4. - P. 731 - 737.
Опубликовано :
ОСОБЕННОСТИ ПОСТУПЛЕНИЯ, ВСАСЫВАНИЯ И УСВОЕНИЯ РАЗЛИЧНЫХ ГРУПП МИКРОЭЛЕМЕНТОВ В ОРГАНИЗМЕ ДЕТЕЙ. Экспериментальная и клиническая гастроэнтерология. 2017;137(01):31-34
Загрузить полный текст
-
- ФГБОУ ВО Первый МГМУ им. И. М. Сеченова Минздрава РФ (Москва, Россия)
Ключевые слова:гастроэзофагеальная рефлюксная болезнь,пищевод Барретта,дети
Резюме:Цель исследования: выявить особенности клинической, эндоскопической и морфологической картины у детей с ГЭРБ с подозрением на пищевод Барретта по данным ЭГДС. Материалы и методы: Первичную группу исследования составили 87 детей, страдающих ГЭРБ. По результатам ЭГДС и гистологического исследования биоптатов слизистой оболочки пищевода у 13 из 87 пациентов были выявлены признаки метаплазии. Эти пациенты составили основную группу исследования. Результаты: У 13 из 87 пациентов с ГЭРБ (14,9%) была выявлена метаплазия слизистой оболочки пищевода (пищевод Барретта): в 10 случаях (11,5%) - по желудочному типу, в 3 (3,4%) - по кишечному типу. По данным ЭГДС, у 6 детей пищевод Барретта был выявлен на фоне эрозивной формы ГЭРБ и у 7 - на фоне неэрозивной ГЭРБ, причем кишечная метаплазия отмечалась только у детей с эрозиями в пищеводе. Клиническая картина у больных с метаплазией эпителия слизистой оболочки пищевода не отличалась от таковой у детей без метаплазии. По данным суточного мониторинга рН у пациентов с пищеводом Барретта в 53,8% случаев определялся физиологический ГЭР, в 38,5% - патологический кислый ГЭР и у одного ребенка (7,7%) - патологический некислотный ГЭР. При этом у всех детей с кишечной метаплазией определялся патологический кислый ГЭР. Выводы: У детей с ГЭРБ возможна метаплазия слизистой оболочки пищевода как по желудочному, так и по кишечному типу. Длительное течение эзофагита, эрозивный эзофагит, патологический кислотный ГЭР предрасполагают к развитию ПБ. Достоверных клинических особенностей течения ПБ у детей с ГЭРБ выявлено не было.
-
- Yousef F., Cardwell C., Cantwell M. M. et al. The incidence of esophageal cancer and highgrade dysplasia in Barrett’s esophagus: a systematic review and meta-analysis // Am J Epidemiol. - 2008. - № 168. - Р. 237 - 249.
- Paull A., Trier J. S., Dalton M. D. et al. The histologic spectrum of Barrett’s esophagus // N. Engl. J. Med. - 1976. - Vol. 295. - P. 476 - 480.
- Shaheen N. Is there a «Barretts Iceberg?» // Gastroenterology. - 2002. - Vol. 123. - № 2. - P. 636 - 638.
- El-Serag H. B., Bailey N. R., Gilger M. A., Rabeneck L. Endoscopic manifestations of gastroesophageal reflux disease in patients between 18 months and 25 years without neurological deficits // Am J Gastroenterol. - 2002. - № 97. - Р. 1635.
- Thomas T., Abrams K. R., DeCaestecker J. S. et al. Meta-analysis: cancer risk in Barrett’s oesophagus // Aliment Pharmacol Ther. - 2007. - № 26. - Р. 1465 - 1477.
- Ивашкин В. Т., Трухманов А. С. Программное лечение гастроэзофагеальной рефлюксной болезни в повседневной практике врача // Российский журнал гастроэнтерологии, гепатологии, колопроктологии. - 2003. - № 6.
- Ивашкин В. Т., Трухманов А. С. Современный подход к терапии гастроэзофагеальной рефлюксной болезни во врачебной практике // РМЖ. - 2003. - № 2. - С. 43 - 48.
- Suzanne M. Jeurnink, Maud Y. A. van Herwaarden-Lindebooma, Peter D. Siersema, Kathelijn Fischer, Roderick H. J. Houwen, David C. van der Zee. Barrett’s esophagus in children: Does it need more attention? // Digestive and Liver Disease. - 2011. - № 43. - Р. 682 - 687.
- Hassall E. Barrett’s esophagus: new definitions and approaches in children // J. Pediatr. Gastroenterol. Nutr. - 1993. - Vol. 16. - № 4. - P 345 - 364.
- Tytgat G. N. Endoscopic cryteries of gastroesophageal reflux // Endoscopy. - 1990. - Vol. 22. - P. 57 - 60.
- Бельмер С. В., Приворотский В. Ф. Гастроэзофагеальная рефлюксная болезнь у детей: отечественный рабочий протокол 2013 года // Лечащий врач. - 2013. - № 8. - С. 66 - 71.
- Vakil N., van Zanten S. V., Kahrilas P., Dent J., Jones R. Global Consensus Group. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus // Am J Gastroenterol. - 2006. - Vol. 101. - № 8. - Р. 1900 - 20.
- DeMeester T. R, Chandrasoma P. Updated guidelines for diagnosis and treatment of gastroesophageal reflux disease // Annu. Rev. Med. - 1999. - Vol. 50. - P. 469 - 506.
- Barrett N. R. Chronic peptic ulcer of the oesophagus and «oesophagitis» // Br J Surg - 1950. - Vol. 38. - P. 175 - 182.
- Allison P. R., Johnston A. S. The oesophagus lined with gastric mucous membrane // Thorax. - 1953. - Vol. 8. - P. 87 - 101.
- Sharma P., McQuaid K., Dent J., Fennerty M. et al. AGA Chicago Workshop. A critical review of the diagnosis and management of Barrett’s esophagus: the AGA Chicago Workshop // Gastroenterology. - 2004. - Vol. 127. - P. 310 - 330.
- Sampliner R. E. and The Practice Parameters Committee of the American College of Gastroenterology. Updated guidelines for the diagnosis, surveillance, and therapy of Barrett’s esophagus // Am J Gastroenterol. - 2002. - № 97. - Р. 1888.
- Giuli R., Siewert J., Couturier D. et al. Barrett’s Esophagus // Paris: John Libbey Eurotext. - 2003. - Vol. l-2.
- Spechler S., Goyal R. The columnar-lined esophagus, intestinal metaplasia and Norman Barrett // Gastroenterology. - 1996. - № 110. - Р. 614 - 621.
- Blot W. J., Devesa S. S., Kneller R. W. et al. Rising incidence of adenocarcinoma of the esophagus and gastric cardia // JAMA. - 1991. - Vol. 265. - P. 1287 - 1289.
- Jankowski J. A., Wright N. A., Meltzer S. J., Triadafllopoulos G. et al. Molecular evolution of the metaplasia-dysplasia-adenocarcinoma sequence in the esophagus //Am J Pathology. - 1999. - Vol. 154. - № 4. - P. 965 - 973.
- Lagergren J., Bergstrom R., Lindgren A., Nyren O. Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma // The New England Journal of Medicine. - 1999. - Vol. 340. - № 11. - Р. 825 - 831.
- Busby W. F., Shuker D. E. G., Charnley G. et al. Carcinogenicity in rats of the nitrosated bile acid conjugates N-nitrosoglycocholic acid and N-nitrosotaurocholic acid // Cancer Res. - 1985. - V. 45. - Р. 1367 - 1371.
- Rector L. E., Connerly M. L. Abberant mucosa in the esophagus in infants and in children // Arch Pathol. - 1941. - № 31. - Р. 285 - 294.
- Darling D. B., Fisher J. H., Gellis S. S. Hiatal hernia and gastoesophageal reflux in infants and children: Analysis of the incidence in North American Children // Pediatrics. - 1974. - № 54. - Р. 450 - 455.
- Hashem B. El-Serag, Mark A. Gilger, Mitchell D. Shub, Peter Richardson, John Bancroft. The prevalence of suspected Barrett’s esophagus in children and adolescents: a multicenter endoscopic study // Gastrointestinal endoscopy. - 2006. - № 5.
- Corley D. A., Kubo A., Levin T. R., Block G., Habel L., Rumore G., Quesenberry C., Buffler P. Race, ethnicity, sex and temporal differences in Barrett’s oesophagus diagnosis: a large community-based study, 1994 - 2006 // Gut. - 2009. - № 58. - Р. 182 - 188.
- Andrici J., Cox M. R., Eslick G. D. Visceral abdominal obesity measured by CT scan is associated with an increased risk of Barrett’s oesophagus: a case-control study // Gut. - 2014. -№ 63. - Р. 220 - 229.
- Avidan B., Sonnenberg A., Schnell T. G., Chejfec G., Metz A., Sontag S. J. The risk of Barrett’s esophagus associated with abdominal obesity in males and females // Int J Cancer. - 2013. - № 132. Р. 2192 - 2199.
- Duggan C., Onstad L., Hardikar S., Blount P. L., Reid B. J., Vaughan T. L. Association between markers of obesity and progression from Barrett’s esophagus to esophageal adenocarcinoma // Clin. Gastroenterol. Hepatol. - 2013. № 11. -Р. 934 - 943.
- Somasundar P., Riggs D., Jackson B., Vona-Davis L., McFadden D. W. Leptin stimulates esophageal adenocarcinoma growth by nonapoptotic mechanisms // Am J Surg. - 2003. -№ 186. -Р. 575 - 578.
- Forssell L., Cnattingius S., Bottai M., Edstedt Bonamy A. K., Lagergren J., Agréus L., Akre O. Increased risk of Barrett’s esophagus among individuals born preterm or small for gestational age // Clin Gastroenterol Hepatol. - 2013. - № 11. Р. 790 - 794.
- Kaijser M., Akre O., Cnattingius S., Ekbom A. Preterm birth, low birth weight, and risk for esophageal adenocarcinoma // Gastroenterology. - 2005. -№ 128. - Р. 607 - 609.
- Crabb D. W., Berk M. A., Hall T. R., Conneally P. M., Biegel A. A., Lehman G. A. Familial gastroesophageal reflux and development of Barrett’s esophagus // Ann Intern Med. - 1985. - № 103. - Р. 52 - 54.
- Jochem V. J., Fuerst P. A., Fromkes J. J. Familial Barrett’s esophagus associated with adenocarcinoma // Gastroenterology. - 1992. -№ 102. - Р. 1400 - 1402.
- Fahmy N., King J. F. Barrett’s esophagus: an acquired condition with genetic predisposition // Am J Gastroenterol. - 1993. - № 88. - Р. 1262 - 1265.
- Eng C., Spechler S. J., Ruben R., Li F. P. Familial Barrett esophagus and adenocarcinoma of the gastroesophageal junction // Cancer Epidemiol Biomarkers Prev. - 1993. - № 2. - Р. 397 - 399.
- Poynton A. R., Walsh T. N., O’Sullivan G., Hennessy T. P. Carcinoma arising in familial Barrett’s esophagus // Am J Gastroenterol. - 1996. - № 91. - Р. 1855 - 1856.
- Chak A., Lee T., Kinnard M. F., Brock W., Faulx A., Willis J. et al. Familial aggregation of Barrett’s oesophagus, oesophageal adenocarcinoma, and oesophagogastric junctional adenocarcinoma in Caucasian adults // Gut. - 2002. - № 51. - Р. 323 - 328.
- Sun X., Elston R., Barnholtz-Sloan J., Falk G., Grady W. M., Kinnard M. et al. A segregation analysis of Barrett’s esophagus and associated adenocarcinomas. Cancer Epidemiol Biomarkers Prev // Am J Gastroenterol. - 2010. - № 19. - Р. 666 - 674.
- Nie S., Chen T., Yang X., Huai P., Lu M. Association of Helicobacter pylori infection with esophageal adenocarcinoma and squamous cell carcinoma: a meta-analysis // Dis. Esophagus. - 2014. - № 27. - Р. 645 - 653.
- Герасимова Н. В., Мызин А. В., Бельмер С. В., Полюдов С. А., Нажимов В. П. Гастроэзофагеальная рефлюксная болезнь у детей как фактор риска аденокарциномы пищевода // ВСП. - 2006. - № 6.
- Au Yeung K. J., Cannon M. L., Arkachaisri T., Gillespie Sand Karnsakul W. Impact of Hiatal Hernia on Pediatric Gastroesophageal Reflux Disease // J Gastrointest. Dig. Sys. - 2015. - № 5. - Р. 5.
- Ивашкин В. Т., Трухманов А. С. Болезни пищевода. Патологическая физиология, клиника, диагностика, лечение. М.: Триада-Х. - 2000. - С. 179.
- Мастыкова Е. К., Конорев М. Р., Матвеенко М. Е. Пищевод Барретта в структуре гастроэзофагеальной рефлюксной болезни: современные представления // Вестник ВГМУ. - 2010. - № 4.
- Буторина Н. В. Опыт лечения детей с гастроэзофагеальной рефлюксной болезнью // 40-я научная сессия ЦНИИГ «Дискуссионные вопросы в гастроэнтерологии». Тезисы докладов. - 2014. - С16.
- Мельченко Д. С., Белова Г. В. Пищевод Барретта: клинико-морфологические сопоставления // Медицинская визуализация. - 2005. -№ 5. - С. 74 - 82.
- Кирова М. В. Конфокальная лазерная эндомикроскопия и уточняющие эндоскопические методики в диагностике пищевода Барретта // ЭиКГ. -2012. - № 4.
- Cameron A. J., Zinsmeister A. R., Ballard D. J., Carney J. A. Prevalence of columnar-lined (Barrett’s) esophagus. Comparison of population-based clinical and autopsy findings // Gastroenterology. - 1990. - № 99. - Р. 918.
- Takubo K., Mafune K., Tanaka Y., Sasajima K. Pathology of cardia // Nippon Gecagakkai Zasshi. - 1998. - № 99. - Р. 547 - 551.
- Lambert R., Sharma P. Paris Workshop on Columnar Metaplasia // Endoscopy. - 2005. - № 37. Р. 879 - 920.
- Van de Bovenkamp J., Porteland-Van Male A., Warson C. et al. // Histopathology. - 2003. - Vol. 42. - P. 86 - 102.
- Рождественская Т. Ю. Ранняя диагностика пищевода Барретта // Электронный научно-образовательный вестник «Здоровье и образование в XXI веке». - 2012. - № 4.
- Пирогов С. С. Эндоскопические методики в уточняющей диагностике и лечении больных с пищеводом Барретта: дисс. канд. мед. наук. - М., 2008. - С. 5 - 197.
- Кирова М. В. Конфокальная лазерная эндомикроскопия и уточняющие эндоскопические методики в диагностике пищевода Барретта // ЭиКГ. -2012. - № 4.
- Коломацкая П. Б. Пищевод Барретта. Эпидемиология, экология, патогенез, морфологическая характеристика, возможности эндоскопической диагностики. Литературный обзор // Вестник РНЦРР. - 2011. - № 11.
Опубликовано :
ОСОБЕННОСТИ ПИЩЕВОДА БАРРЕТТА У ДЕТЕЙ. Экспериментальная и клиническая гастроэнтерология. 2017;137(01):35-43
Загрузить полный текст
-
- СПб ГБУЗ «Детская городская поликлиника № 8», Консультативно диагностический центр со стационаром дневного пребывания, Минздрава России (Санкт-Петербург, Россия)
- СПб ГБУЗ «Городская поликлиника № 23», Консультативно диагностический центр для детей № 2, Минздрава России (Санкт-Петербург, Россия)
Ключевые слова:дети, СИБР, заболевания жкт
Резюме:В статье изложены клинико-анамнестические особенности у детей с синдромом избыточного бактериального роста (СИБР), диагностированным методом дыхательного теста с лактулозой. Выявлено, что среди детей с СИБР достоверно чаще встречалась функциональная диспепсия, лактазная недостаточность. При этом клиническая картина СИБР у детей оказалась неспецифична, однако пробиотическая терапия оказывала выраженный терапевтический эффект.
-
- Вялов С. С. Синдром избыточного бактериального роста: особенности патогенеза иммунных нарушений // РМЖ. - 2014. - № 15. - С. 1083
- Нижевич А. А. Синдром избыточного бактериального роста в детском возрасте / Нижевич А. А., Алянгин В. Г., Астрелина Е. М., Королева Е. Г., Ханнанова Г. Б., Акбашев Р. Н., Якупова Г. М // РМЖ. - 2014. - № 15. - С. 1094
- Цех О. М., Новикова В. П. Синдром избыточного бактериального роста // Педиатр. - 2010. - Т. 1, № 1. - С. М54-М59.
- Белоусова Е. А. Синдром избыточного бактериального роста в тонкой кишке в свете общей концепции о дисбактериозе кишечника: взгляд на проблему // Фарматека. - 2009. - № 2. - С. 10 - 11.
- Singh V. V., Toskes P. P. Small Bowel Bacterial Overgrowth: Presentation, Diagnosis, and Treatment // Curr Treat Options Gastroenterol. - 2004 - 7 (1). - Р. 19 - 28.
- Quigley E. M., Abu-Shanab A. Small intestinal bacterial overgrowth // Infect Dis Clin North Am. - 2010. - V. 24. - Р. 943.
- Микрофлора пищеварительного тракта / под ред. Хавкина А. И. - Москва.: Фонд социальной педиатрии. - 2006. - 416 с.
- Микробиота желудочно-кишечного тракта при хроническом гастрите / под ред. А. Н. Суворова, В. П. Новиковой, И. Ю. Мельниковой. - Москва.: ИнформМед. - 2014. - 210с.
- Урсова Н. И. Дисбактериозы кишечника в детском возрасте: инновации в диагностике, коррекции и профилактике. Руководство для врачей. Москва. - 2013. - 328с.
- Новикова В. П. Состояние микрофлоры тонкой кишки при хроническом гастродуодените / Новикова В. П., Цех О. М., Оришак Е. А., Барышникова Н. В. // Вопросы практической педиатрии. - 2009. - Т. 4, № 4. - С. 14 - 19.
- Mello C., Tahan S., Melli L. et al. Methane production and small intestinal bacterial overgrowth in children living in a slum // World J. Gastroenterol. 2012. - Vol. 18. - Р. 5932 - 5939.
- Pereira S., Khin-Maung-U. T., Duncombe V. et al. A pattern of breath hydrogen excretion suggesting small bowel bacterial overgrowth in Burmese village children // J. Pediatr. Gastroenterol. Nutr. - 1991 -. Vol. 13. - Р. 32 - 38.
- Цех О. М, Новикова В. П. Синдром избыточного бактериального роста и функциональное состояние слизистой двенадцатиперстной кишки у детей с хроническим гастродуоденитом // Материалы четвертой Российской научно-практической конференции «Воронцовские чтения. Санкт-Петербург-2011». - СПб., 2011. - С. 75 - 79.
- Malik B., Xie Y., Wine E., Huynh H. Diagnosis and pharmacological management of small intestinal bacterial overgrowth in children with intestinal failure // Can. J. Gastroenterol. - 2011. - Vol. 25. - Р. 41 - 45.
- Pereira S., Khin-Maung-U. T., Duncombe V. et al. A pattern of breath hydrogen excretion suggesting small bowel bacterial overgrowth in Burmese village children // J. Pediatr. Gastroenterol. Nutr. - 1991. - Vol. 13. - Р. 32 - 38.
- Shelley H., Brennan M., Heuschkel R. Hydrogen breath testing in children: what is it and why is it performed? // Gastroint. Nurs. - 2009. - Vol. 7. - Р. 18 - 27.
- E. Scarpellini, V. Giorgio, M. Gabrielli et al. Rifaximin treatment for small intestinal bacterial overgrowth in children with irritable bowel syndrome: a preliminary study // Eur. Rev. Med. Sci. - 2013. - Vol. 17. - Р. 1314 - 1320.
- Lisowska A., Wojtowicz J., Walkowiak J. Small intestine bacterial overgrowth is frequent in cystic fibrosis: combined hydrogen and methane measurements are required for its detection // Acta Biochim. Pol. - 2009. - Vol. 56. - Р. 631 - 634.
- Новикова В. П., Калинина Е. Ю., Шабалов А. М., Осмаловская Е. А. Лямблиоз: Учебное пособие для врачей. / Санкт-Петербург: ИнформМед. - 2010. - 120 с.
- Ардатская М. Д. Диагностическое значение содержания короткоцепочечных жирных кислот при синдроме раздраженного кишечника //Рос. журн. гастроэнтерол., гепатол. и колопроктол. - 2000. -Т. 10, № 3. - С. 36 - 41.
- Методика масс-спектрометрии микробных маркеров как способ оценки пристеночной кишечной микробиоты при заболеваниях органов пищеварения. / Учебно-методическое пособие под редакцией Г. А. Осипова, В. П. Новиковой, Санкт-Петербург: Левша. - 2013. - 96с.
- Мубаракшина О. А Избыточный бактериальный рост в кишечнике: особенности патогенеза и фармакотерапии // Медицинский вестник. - 2008. - № 19. - С. 446
- Toskes P. P., Donaldson R. M. Enteric bacterial flora and bacterial overgrowth /In: Sleisinger & Fortrand’s Gastrointestinal Diseases, Fifth Edition. Eds., Feldman M, Scharschmitt B. F., Sleisinger M. H. - 1993. -Р. 1106 - 1117.
- Мельникова И. Ю., Новикова В. П. Методы исследования кишечника у детей и подростков. Учебно-методическое объединение по медицинскому и фармацевтическому образованию. - Санкт-Петербург, 2006. - 82 с.
- Новикова В. П. Методы исследования органов пищеварения. Гастроэнтерология: руководство для врачей /под ред. Е. И. Ткаченко. - Санкт-Петербург: Издательство СпецЛит. - 2013. - С. 16 - 83.
- Корниенко Е. А. Клиническое применение водородного дыхательного теста в диагностике лактазной недостаточности и синдрома избыточного бактериального роста у детей раннего возраста / Корниенко Е. А., Кубалова С. С., Дмитриенко М. А., Джагацпанян И. Э. // Педиатр. - 2013. - № 4. - С. 9 - 15.
- Eisenmann A., Amann A., Said M. et al. Implementation and interpretation of hydrogen breath tests // J. Breath Res. - 2008. - Vol. 2. - 046002 (9 рр.).
- Corazza G. R., Menozzi M. G., Strocchi A., et al. The diagnosis of small bowel bacterial overgrowth. Reliability of jejunal culture and inadequacy of breath hydrogen testing // Gastroenterology. - 1990 - Vol.98. - Р. 302.
- Riordan S. M., McIver C. J., Walker B. M., et al. The lactulose breath hydrogen test and small intestinal bacterial overgrowth // Am J Gastroenterol. - 1996. - Vol. 91. - Р. 1795.
- Kerlin P., Wong L. Breath hydrogen testing in bacterial overgrowth of the small intestine // Gastroenterology. - 1988. -Vol.95. - Р. 982.
- Rana S. V., Sharma S., Kaur J., et al. Comparison of lactulose and glucose breath test for diagnosis of small intestinal bacterial overgrowth in patients with irritable bowel syndrome // Digestion. - 2012. - Vol. 85. - Р. 243.
- Козлов А. В. Газоанализатор «Helico Sense» как новое средство для диагностики хелико- бактерной инфекции / Евстратова Ю. С., Новикова В. П., Ткаченко Е. И., Хочинская О. Ю. //Медицинская техника. - 2006. № 3. - С. 44 - 46.
- Bohm M., Siwiec R. M., Wo J. M. Diagnosis and management of small intestinal bacterial overgrowth // Nutr. Clin. Pract. - 2013. - Vol. 28 (3). - P. 289 - 299.
- Gasbarrini A., Lauritano E. C., Gabrielli M. et al. Small intestinal bacterial overgrowth: diagnosis and treatment // Dig. Dis. Sci. - 2007. - Vol. 25. - P. 237 - 240
- Smallin testinal bacterial overgrowth syndrome / J. Bures, J. Cyrany, D. Kohoutova [et al.] // World. J. Gastroenterol. - 2010. - Vol. 16. - P. 2978 - 90.
- Денисенко Т. Л. Диагностика СИБР у больных с хеликобактер-ассоциированной гастродуоденальной патологией / Т. Л. Денисенко, К. М. Перфилова, Н. В. Неумоина, И. В. Шутова, М. В. Неумоина, Е. И. Ефимова// Микробиология и эпидемиология Вестник Нижегородского университета им. Н. И. Лобачевского. - 2012. - № 2 (3). - С. 41 - 44.
- Ручкина И. Н. Роль микрофлоры тонкой кишки в развитии вторичной лактазной недостаточности и возможности ее лечения / Ручкина И. Н., Фадеева Н. А., Парфенов А. И., Щербаков П. Л., Губина А. В., Полева Н. И., Хомерики С. Г. // Терапевтический архив. - 2013. - № 2. - С. 21 - 26.
- Mayevskaya Yе. А., Cheryomushkin S. V., Krivoborodova N. A., Kucheryavy Yu. A. Bacterial overgrowth syndrome in the small intestine: from recent scientific data to routine practice // Klin. perspektivy gastroenterol. gepatol. - 2013. - N 5. - P. 30 - 41.
- Yu D., Cheeseman F., Vanner S. et al. Combined orocaecal scinthigraphy and lactulose hydrogen breath testing demonstrate that breath testing detects orocaecal transit, not small intestinal bacterial overgrowth in patients with IBS // Gut. - 2011. - Vol. 60 (3). - P. 334 - 340.
- Choung R. S., Ruff K. C., Malhotra A. et al. Clinical predictors of small intestinal bacterial overgrowth by duodenal aspirate culture // Aliment. Pharmacol. Ther. - 2011. - Vol. 33 (9). -P. 1059 - 1067
- Madrid A. M., Poniachik J., Quera R., Defilippi C. Small intestinal clustered contractions and bacterial overgrowth: a frequent finding in obese patients // Dig Dis Sci. -2011. - N 56. - Р: 155 - 60.
- Кучерявый Ю. А. Взаимосвязь синдромов раздраженного кишечника и избыточного бактериального роста: есть ли она? / Кучерявый Ю. А., Черемушкин С. В., Маевская Е. А., Сутугина Е. А. // Росс журн гастроэнтерол гепатол колопроктол. -2014. - N2. - Р. 5 - 14.
Опубликовано :
6.СИНДРОМ ИЗБЫТОЧНОГО БАКТЕРИАЛЬНОГО РОСТА ПРИ ЗАБОЛЕВАНИЯХ ЖЕЛУДОЧНО-КИШЕЧНОГО ТРАКТА У ДЕТЕЙ. Экспериментальная и клиническая гастроэнтерология. 2017;137(01):44-48
Загрузить полный текст
-
- ГБОУ ВПО ПГМУ им. академика Е. А. Вагнера Минздрава России (Пермь, Россия)
- ГБУЗ ПК «Пермская краевая клиническая инфекционная больница» (Пермь, Россия)
Ключевые слова:ротавирусная инфекция,дети,иммуноферментный анализ,прогноз,тяжелая форма заболевания,коэффициент позитивности
Резюме:В статье анализируется возможность прогнозирования развития тяжелых форм ротавирусной инфекции (РВИ) у госпитализированных детей раннего возраста с помощью первичного лабораторного обследования. В качестве прогностического критерия предлагается использовать коэффициент позитивности (КП), вычисляемый при проведении иммуноферментного анализа (ИФА) тест-системы «Ротавирус-антиген-ИФА-БЕСТ» (г. Новосибирск) в первые сутки госпитализации. Разработан алгоритм определения порогового разделяющего значения коэффициента. Определена вероятность развития тяжелых форм РВИ у детей раннего возраста, в 3,5 раза превышающая показатель, установленный клинически. Если методом ИФА (тест-система «Ротавирус-антиген-ИФА-БЕСТ») определяется значение КП ≥ 13, и мы допускаем априорную вероятность тяжелого течения болезни равной 0,24, то вероятность развития тяжелых форм РВИ у детей раннего возраста составит 0,84 (т. е. 84%), что в 3,5 раза превышает показатель, установленный клинически. С учетом получения ответа ИФА из фекалий ребенка в первый день госпитализации прогноз вероятности тяжелой формы РВИ может служить обоснованием ранней терапии иммуноглобулинами для внутривенного введения. Выводы: 1. У госпитализированных детей раннего возраста с верифицированной ротавирусной инфекцией в 24,0% случаев диагностированы тяжелые формы заболевания. 2. Коэффициент позитивности оптической плотности, вычисляемый при проведении иммуноферментного анализа тест-системой «Ротавирус-антиген-ИФА-БЕСТ» г. Новосибирск, может служить мерой вероятности развития тяжелых форм ротавирусной инфекции у детей раннего возраста - его значения при тяжелых формах выше, чем при среднетяжелых 16,7 > 9,2 (t=0,97, p=0,00). 3. При значениях коэффициента позитивности более 13, вероятность развития тяжелой формы заболевания составляет 84%.
-
- Денисюк Н. Б. Современные аспекты лабораторной диагностики и профилактики ротавирусной инфекции у детей //Журнал инфектологии. 2015. Том 7. № 1. С. 31 - 37.
- Ливицкая Н. И., Кувшинова И. Н, Рукавишников М. Ю. Ротавирусная инфекция и ее диагностика. // Новосибирск Информационный Бюллетень ЗАО «Вектор-Бест». 2008. 2 (48). С 1 - 4.
- Иволгина А. В., Молочный В. П. Клинические особенности вирусных диарей у детей первого года жизни. // Дальневосточный Журнал Инфекционной Патологии. 2008. № 12. С. 32 - 34.
- Подколзин А. Т., Гусева А. Н., Веселова О. А., Курочкина Д. Е., Шипулин Г. А. Сравнительная характеристика наборов реагентов для выявления антигенов ротавирусов, используемых на территории России. //Клиническая лабораторная диагностика. 2015 № 6. С 48 - 52.
- Ribas, M. A.,Tejero, Y., Cordero, Y., de los Angeles León, M., Rodriguez, M., Perez-Lastre, J., Triana, T., Guerra, M., Ayllón, L., Escalante, G., Hadad, J. Detection of rotavirus and other enteropathogens in children hospitalized with acute gastroenteritis in Havana, Cuba. // Archives of Virology Volume 160, Issue 8, 31 May 2015, Pages 1923 - 1930
- R. Zhou, J. L. Xu, D. Wu and J. L. Tang. Analysis of prognostic factors for infantile rotavirus infection. //Genetics and Molecular Research. Volume 14, Issue 1, 2 February 2015, Pages 790 - 796.
Опубликовано :
ПРОГНОЗИРОВАНИЕ ТЯЖЕЛОГО ТЕЧЕНИЯ РОТАВИРУСНОЙ ИНФЕКЦИИ У ДЕТЕЙ РАННЕГО ВОЗРАСТА. Экспериментальная и клиническая гастроэнтерология. 2017;137(01):49-52
Загрузить полный текст
-
- Федеральное государственное бюджетное учреждение «Детский научно-клинический центр инфекционных болезней Федерального медико-биологического агентства» (Санкт-Петербург, Россия)
- ФБУН Санкт-Петербургский НИИ эпидемиологии и микробиологии им. Пастера МЗ РФ (Санкт-Петербург, Россия)
- Северо-Западный государственный медицинский университет им. И. И. Мечникова (Санкт-Петербург, Россия)
- ФГБНУ «ИЭМ» (Санкт-Петербург, Россия)
- Санкт-Петербургский государственный университет (Санкт-Петербург, Россия)
Ключевые слова:ротавирусная инфекция,норовирусная инфекция,дисбиоз кишечника,синдром избыточного бактериального роста
Резюме:Цель работы: изучение микробиоты кишечника у детей с вирусными кишечными инфекциями (ВКИ) и определение роли дисбиотических расстройств в генезе функциональной патологии органов пищеварения (ФПОП). Материалы и методы. Наблюдали 143 пациента в возрасте от 1 до 7 лет, без гастроэнтерологической патологии в анамнезе со среднетяжелой ротавирусной (РВИ), норовирусной (НВИ) и смешанной рота-норовирусной (РНВИ) кишечными инфекциями, верифицированными методом ПЦР в фекалиях. Микробиоту кишечника оценивали бактериологическим методом и с помощью ПЦР в реальном времени а также с помощью водородного дыхательного теста (исследование на наличие синдрома избыточного бактериального роста). В течение 1 года осуществлялось катамнестическое наблюдение для выявления функциональных заболеваний органов пищеварений Результаты. В остром периоде РВИ обнаружено достоверное снижение Bacteroides thetaiataomicron. и увеличение Bacteroides fragilis по сравнению с НВИ. Пролиферация УПМ отмечалась у четверти больных ВКИ и сопровождалась воспалительными изменениями в копрограмме, более часто при РНВИ. ФПОП диагностирована у 22,7% реконвалесцентов ВКИ, частота которой была ниже в случае НВИ по сравнению с РВИ и РНВИ. У детей, сформировавших ФПОП, в составе микробиоты кишечника выявлена тенденция к снижению Bifidobacterium spp., F. prausnitzii и увеличению B. fragilis в периоде реконвалесценции ВКИ. СИБР диагностирован во всех группах, с максимальной частотой при РНВИ (54,5%). Выявлена связь СИБР с манифестацией ФПОП. Заключение. Дисбиоз кишечника и СИБР при ВКИ патогенетически связаны с развитием постинфекционной ФПОП у детей.
-
- World Health Organization. World health statistics 2010. - World Health Organization, 2010.
- Ahmed S. M., Hall A. J., Robinson A. E. et al. Global prevalence of norovirus in cases of gastroenteritis: a systematic review and meta-analysis. Lancet Infect. Dis. 2014; 14 (8): 725 - 30.
- Lanata C. F., Fischer-Walker C. L., Olascoaga A. C. et al. Child health epidemiology reference group of the World Health Organization and UNICEF global causes of diarrheal disease mortality in children younger 5 years of age: a systematic review. PLoS One. 2013; 8 (9): e72788.
- Nataro J. P. Hot topics in infection and immunity in children. In: Diarrhea among children in developing countries. Springer: New York, 2013. IX; p. 73 - 80.
- Spiller R., Lam C. An update on post-infectious irritable bowel syndrome: role of genetics, immune activation, serotonin and altered microbiome. J. Neurogastroenterol. Motil. 2012; 18 (3): 258 - 68.
- Thabane M., Kottachchi D. T., Marshall J. K. Systematic review and meta-analysis: The incidence and prognosis of post-infectious irritable bowel syndrome. Aliment. Pharmacol. Ther. 2007; 26 (4): 535 - 44.
- Thabane M., Simunovic M., Akhtar-Danesh N. et al. An outbreak of acute bacterial gastroenteritis is associated with an increased incidence of irritable bowel syndrome in children. Am. J. Gastroenterol. 2010; 105 (4): 933 - 9.
- Saps M., Pensabene L., Turco R., Staiano A. et al. Rotavirus gastroenteritis: precursor of functional gastrointestinal disorders? J. Pediatr. Gastroenterol. Nutr. 2009; 49 (5): 580 - 3.
- Moon C., Stappenbeck T. S. Viral interactions with the host and microbiota in the intestine. Curr. Opin. Immunol. 2012; 24 (4): 405 - 10.
- Дисбиоз кишечника. Руководство по диагностике и лечению / под ред. Е. И. Ткаченко, А. Н. Суворова. СПб: ИнформМед. 2009. 267 с.
- Drossman D. A., Dumitrascu D. L. Rome III: New standard for functional gastrointestinal disorders. J Gastrointestin. Liver Dis. 2006; 15 (3):237 - 41.
- Borgaonkar M. R., Ford D. C., Marshall J. K. et al. The incidence of irritable bowel syndrome among community subjects with previous acute enteric infection. Dig Dis Sci. 2006; 51:1026 - 32.
- Корниенко Е. А., Типикина М. Ю. Роль воспалительных и микробиологических изменений в патогенезе функциональных расстройств кишечника у детей. Вопр. детс. диетол. 2012; 3: 76 - 8.
- Думова Н. Б. Функциональные заболевания органов пищеварения у детей. В: Детская гастроэнтерология: руководство для врачей / под ред. Н. П. Шабалова. М.: МЕД пресс-информ, 2013.
- Wu S., Rhee K.-J., Zhang M. et al. Bacteroides fragilis toxin stimulates intestinal epithelial cell shedding and γ-secretase-dependent E-cadherin cleavage. J. Cell Sci. 2007; 120: 1944 - 52.
- Wrzosek L., Miquel S., Noordine M. L. et al. Bacteroides thetaiotaomicron and Faecalibacterium prausnitzii influence the production of mucus glycans and the development of goblet cells in the colonic epithelium of a gnotobiotic model roden. bmc Biol. 2013; 11 (1): 1 - 13.
- Михайлова Е. В., Левин Д. Ю., Данилов А. Н., Кошкин А. П., Лаврентьев Г. П. Ротавирусная инфекция у детей: клинико-лабораторная характеристика и катамнестические данные. Саратовский научно-медицинский журнал. 2013; 9 (3): 504 - 508.
- Подколзин, А. Т., Петухов, Д. Н., Веселова, О. А., Коновалова, Т. А., Чернявская, О. П., Морозова, Н. С., & Черепанова, Е. А. Позитивные и проблемные аспекты применения ротавирусных вакцин. Эпидемиология и вакцинопрофилактика. 2013 (1), 68: 80 - 89.
- Singer, C., Stancu, P. O. L. I. X. E. N. I. A., Coşoveanu, S., Osiac, L. O. R. E. D. A. N. A., Grigorie, C. O. C. A., & Botu, A. L. I. N. A. Diarrhea with Rotavirus in Children. Current Health Sciences J. 2010; 36: 5698, 700: 240 - 244.
- Varyukhina S., Freitas M., Bardin S. et al. Glycan-modifying bacteria-derived soluble factors from Bacteroides thetaiotaomicron and Lactobacillus casei inhibit rotavirus infection in human intestinal cells. Microbes Infec. 2012; 14 (3): 273 - 8.
- Мескина Е. Р. Особенности микробиоты у детей с отягощенным преморбидным состоянием при вирусных диареях. Способы коррекции нарушений. РМЖ, 2011; 18: 1126 - 30.
- Кветная А. С., Железова Л. И. Этиопатогенетические механизмы формирования дисбиоза просвета толстой кишки при острых кишечных инфекциях у детей. Профилакт. медиц. 2008; 3 (28): 41 - 3.
Опубликовано :
НАРУШЕНИЕ МИКРОБИОЦЕНОЗА КИШЕЧНИКА КАК ФАКТОР ФОРМИРОВАНИЯ ПОСТИНФЕКЦИОННОЙ ПАТОЛОГИИ ОРГАНОВ ПИЩЕВАРЕНИЯ У ДЕТЕЙ ПОСЛЕ ВИРУСНЫХ КИШЕЧНЫХ ИНФЕКЦИЙ. Экспериментальная и клиническая гастроэнтерология. 2017;137(01):53-57
Read & Загрузить полный текст
-
- ФГАУ «Научный центр здоровья детей» Министерства здравоохранения Российской Федерации (Москва, Россия)
- Научно-исследовательский клинический институт педиатрии Российского национального исследовательского медицинского университета им. Н. И. Пирогова (Москва, Россия)
- ГБОУ ВПО РНИМУ им. Н. И. Пирогова (Москва, Россия)
Ключевые слова:дети,наследственная тирозинемия I типа,специфическая терапия,нарушения функции печени,пошаговая диагностика
Резюме:Введение: Тирозинемия I типа - редкое генетическое заболевание, приводящее к развитию цирроза печени, печеночной недостаточности и тубулопатии. В связи с этим огромное значение имеет ранняя диагностика и своевременное начало патогенетического лечения заболевания. Цель. На основе многофакторного статистического анализа клинико-диагностических показателей и их изменений в динамике разработать алгоритм пошаговой диагностики наследственной тирозинемии I типа у детей и оценить эффективность патогенетической терапии. Объём и методы. Под наблюдением находились 17 детей (8 мальчиков и 9 девочек) с тирозинемией I типа: 5 пациентов (29,4%) с IA типом и 12 пациентов (70,6%) с IБ типом. Все дети получали патогенетическую терапию нитизиноном. Проводилось изучение анамнеза жизни и заболевания пациентов, оценивались клинико-лабораторные данные в дебюте заболевания и на фоне шестимесячного курса патогенетической терапии. Результаты. С помощью многофакторного статистического анализа выявлены клинико-лабораторные критерии диагностики тирозинемии 1 типа у детей раннего возраста с последующим составлением пошагового алгоритма диагностики заболевания. Проведена оценка выраженности нарушения функции печени до и через 6 месяцев после начала специфической терапии, которая доказала её улучшение.
-
- Tyrosinemia, Type I (OMIM). Available at: http://omim.org/entry/276700
- http://ghr.nlm.nih.gov/condition/tyrosinemia www.omim.org/entry/276700
- Kvittingen E. A., Rootwelt H., Brandtzaeg P., Bergan A., Bergen R. Hereditary tyrosinemia type 1. Self-induced correction of the fumarylacetoacetase defect. J. Clin. Invest. 1993; v. 91 (4): p. 1816 - 1821.
- Goldsmith L. A., Laberge C. Tyrosinemia and related disorders. In: Scriver C. R., Beaudet A. L., Sly W. L., Valle D., eds. The metabolic basis of inherited diseases. 1989; 6-th ed: p. 547 - 562.
- Holme E., Lindstedt S. Diagnosis and management of tyrosinemia type I. Curr Opin Pediatr. 1995; 7:726 - 32.
- Tyrosinemia Type 1. National Organization for Rare Disorders. Available at: http://www.rarediseases.org/rare-disease-information/rare-diseases/byID/446/viewAbstract
- Van Spronsen F. J., Thomasse Y., Smit G. P., Leonard J. V., Clayton P. T., Fidler V., et. al. Hereditary tyrosinemia type I: a new clinical classification with difference in prognosis on dietary treatment. Hepatology. 1994; 20: 1187 - 91
- Larochelle J., Alvarez F., Bussieres J. F., Chevalier I., Dallaire L., Dubois J., et. al. Effect of nitisinone (NTBC) treatment on the clinical course of hepatorenal tyrosinemia in Quebec. Mol. Genet. Metab. 2012; 107: 49 - 54.
- Nitisinone in the treatment of hereditary tyrosinaemia type 1. Drugs. 2006;66:743 - 50. [PubMed] [Reference list]
- Masurel-Paulet A., Poggi-Bach J., Rolland M. O., Bernard O., Guffon N., Dobbelaere D., at al. NTBC treatment in tyrosinaemia type 1: long-term outcome in French patients. J. Inherit. Metab. Dis. 2008; 31: 81 - 7.
- Maiorana A., Malamisura M., Emma F., Boenzi S., Di Ciommo V. M., Dionisi-Vici. Early effect of NTBC on renal tubular dysfunction in hereditary tyrosinemia type 1. C. Mol Genet Metab. 2014 Nov; 113 (3): 188 - 93.
- Holme E., Lindstedt S., Van Spronsen F. J., Berger R., Smit G. P. et al. Tyrosinaemia type I: orthotopic liver transplantation as the only definitive answer to a metabolic as well as an oncological problem. J. Inherit. Metab. Dis. 1989; 12 (2): 339 - 342.
- Евлюхина Н. Н., Волынец Г. В., Филин А. В., Пахомовская Н. Л. Динамика степени нарушения функции печени при болезни Вильсона и аутоиммунном гепатите у детей. Российский журнал гастроэнтерологии, гепатологии, колопроктологии: Материалы девятнадцатого Российского конгресса «Гепатология сегодня». 2014; 24 (1): 63.
- Волынец Г. В., Потапов А. С., Полякова С. И., Александров А. Е., Сенякович В. М., Сурков А. Н., Четкина Т. С., Евлюхина Н. Н., Скворцова Т. А. Определение степени нарушения функции печени у детей. Вопросы современной педиатрии. 2013; 12 (4): 47 - 51.
- Волынец Г. В., Евлюхина Н. Н., Потапов А. С., Хавкин А. И., Филин А. В., Сурков А. Н., Пахомовская Н. Л., Скворцова Т. А. Определение степени нарушения функции печени у детей с позиций международной классификации функционирования, ограничений жизнедеятельности и здоровья (МКФ). Экспериментальная и клиническая гастроэнтерология. 2015; 7 (119): 31 - 37.
- Волынец Г. В., Евлюхина Н. Н., Филин А. В., Потапов А. С., Дворяковский И. В., Дворяковская Г. М., Сурков А. Н., Шавров А. А., Пахомовская Н. Л., Скворцова Т. А. Структура и функция печени и их нарушения при хронических болезнях гепатобилиарной системы у детей. Вестник Российской академии медицинских наук. 2015; 70 (2): 203 - 213.
- Власов, В. В. Эффективность диагностических исследований. Москва: Медицина; 1988; 253.
Опубликовано :
АЛГОРИТМ ПОШАГОВОЙ ДИАГНОСТИКИ И ДИНАМИКА ИЗМЕНЕНИЙ СТРУКТУРЫ И ФУНКЦИИ ПЕЧЕНИ НА ФОНЕ СПЕЦИФИЧЕСКОЙ ТЕРАПИИ ТИРОЗИНЕМИИ I ТИПА У ДЕТЕЙ. Экспериментальная и клиническая гастроэнтерология. 2017;137(01):58-64
Загрузить полный текст
-
- Государственное бюджетное образовательное учреждение высшего профессионального образования министерства здравоохранения Российской Федерации «Нижегородская медицинская академия» (Нижний Новгород, Россия)
- Государственное бюджетное образовательное учреждение высшего профессионального образования министерства здравоохранения Российской Федерации «Первый московский медицинский университет им. И. М. Сеченова» (Москва, Россия)
- Государственное бюджетное образовательное учреждение высшего профессионального образования министерства здравоохранения Российской Федерации «Северо-западный государственный медицинский университет им. И. И. Мечникова» (Санкт-Петербург, Россия)
Ключевые слова:дети,острый вирусный гепатит В,гастрин сыворотки крови
Резюме:Цель изучения - уровень гастрина сыворотки крови у детей при лёгкой форме гепатита В, его влияние на клиническое течение болезни. Материал и методы исследования. Обследованы 48-и детей в возрасте от 3-х до 15-и лет по стандарту вирусных гепатитов с определением в сыворотке крови дополнительно утреннего гастрина. В первую группу вошли 33 ребёнка, больных лёгкой формой гепатита В. Группу сравнения (норму) составили 15 здоровых детей. Результаты исследований. У большинства детей (69,7%), больных лёгкой формой гепатита В, в сыворотке крови, по сравнению со здоровыми детьми (нормой), имели место повышенные показания гастрина, подтверждаемые результатами эзофагогастродуоденоскопии (ЭГДС) как функциональная диспепсия. Выводы 1. Желтушные формы ГВ у детей, начиная с лёгкой формы болезни, в большинстве случаях сопровождаются функциональной диспепсией. 2. Желтушные формы ГВ у детей, начиная с лёгкой формы болезни, следует лечить как патологию печени, сопровождающуюся функциональной диспепсией, что позволит повысить эффективность их терапии. 3. Диспансерное наблюдение и реабилитацию детей, перенесших желтушные формы ГВ, начиная с лёгкой формы болезни, врачу-инфекционисту необходимо проводить совместно с врачом-гастроэнтерологом; это обеспечит своевременное выявление у них гастродуоденальной патологии и положительно повлияет на увеличение доли здоровых детей.
-
- Климов П. К., Барашкова Г. М. Физиология желудка. Механизмы регуляции. - Л.: Наука. - 1991. - 256 с.
- Щербаков П. Л. Современные проблемы подростковой гастроэнтерологии. //Педиатрия. - 2010. - Т. 89. - № 2. - С. 6 - 11.
- Arkachaisri T. Serum sickness and hepatitis B vaccine including review of the literature. //J. Med. Assoc. Thai. - 2002. - Aug.; - 85 Suppl - 2: - S 607 - 12.
- Шагинян В. Р., Гураль А. Л., Сергеева Т. А. и соавт. Иммунологическая и эпидемиологическая эффективность вакцинации против гепатита В: результаты многоцентрового исследования. //Эпидемиология и инфекционные болезни: актуальные вопросы. - 2013. - № 4. - С. 20 - 26.
- Лобзин Ю. В. Скрипченко Н. В., Бехтерева М. К. и соавт. Проблемы детских инфекций на современном этапе. //Инфекцион. бол. - 2009. - Т. 7 - № 2 - С. 7 - 12.
- Маев И. В., Мельникова Е. В., Крюкова Т. В. и др. Новые методы серологической и эндоскопической диагностики хронического атрофического гастрита и раннего рака желудка. //Клинические перспективы гастроэнтерологии, гепатологии. - 2009. - № 6. - С. 30 - 34.
- Morisset J., Laine J., Biernat M. et al. What are the pancreatic target cells for gastrin and its CCKB receptor? Is this a couple for cancerous cells? //Med. Sci Monit. - 2004. - Vol. 10. - № 10. - Р. 242 - 246.
- Konturek S. J., Gonciarz M., Gonciarz Z. et al. Progastrin and its products from patients with chronic viral hepatitis and liver cirrhosis. //Scand J. Gastroenterol. - 2003. - Vol. 38. - № 6. - Р. 643 - 647.
- Пайков В. Л., Соколова М. И., Муравьева Н. Н. и др. Роль вирусных гепатитов в формировании хронических заболеваний органов пищеварения в детском возрасте. //Дет. гастроэн. и пробл. педиатр вчера, сегодня, завтра. Сб. науч. тр. - Н. Новгород. - 1999. - С. 95 - 96.
- Блюгер А. Ф., Новицкий И. Н. Вирусные гепатиты. - Рига. - Звайгэне.-1988. - 414 с.
Опубликовано :
ВЛИЯНИЕ ГАСТРИНЕМИИ НА КЛИНИЧЕСКОЕ ТЕЧЕНИЕ ОСТРОГО ВИРУСНОГО ГЕПАТИТА В У ДЕТЕЙ. Экспериментальная и клиническая гастроэнтерология. 2017;137(01):65-67
Загрузить полный текст
-
- РНИМУ им. Н. И. Пирогова (Москва, Россия)
Ключевые слова:дефицит кислой лизосомальной липазы,болезнь накопления эфиров холестерина,дислипидемия,гепатомегалия,Болезнь Вольмана
Резюме:Болезнь Вольмана или дефицит кислой лизосомальной липазы - редкое аутосомно-рецессивное заболевание, вызванное повреждающими мутациями гена LIPA. Возраст начала заболевания и темпы его прогрессирования вариабельны и обусловлены характером мутаций. Заболевание у детей грудного возраста характеризуется быстро прогрессирующим течением и проявлением и симптомов в первые недели жизни и даже внутриутробно. Эти пациенты редко доживают до 6 месяцев. У детей старшего возраста заболевание характеризуется сочетанием дислипидемии, гепатомегалии, повышением уровня трансаминаз и микровезикулярным стеатозом в биопсийном материале. У пациентов наблюдается повреждение печени с исходом в фиброз, цирроз, повышением уровней холестерина липопротеинов низкой плотности и снижение уровней холестерина липопротеинов высокой плотности. Уже в детском возрасте могут проявляться и признаки поражения сердечно-сосудистой системы. В обзоре представлены данные о перспективах заместительной ферментной терапии препаратом себелипаза альфа, представляющим собой рекомбинантную человеческую кислую лизосомальную липазу.
-
- Bernstein DL, Hulkova H, Bialer MG, Desnick RJ. Cholesteryl ester storage disease: review of the findings in 135 reported patients with an underdiagnosed disease. J Hepatol 2013;58:1230 - 43.
- Hulkova H, Elleder M. Distinctive histopathological features that support a diagnosis of cholesterol ester storage disease in liver biopsy specimens. Histopathology 2012;60:1107 - 13.
- Abramov A, Schorr S, Wolman M. Generalized xanthomatosis with calcified adrenals. AMA J Dis Child 1956;91:282 - 6.
- Fredrickson DS. Newly recognized disorders of cholesterol metabolism. Ann Intern Med 1963;58:718.
- Burke JA, Schubert WK. Deficient activity of hepatic acid lipase in cholesterol ester storage disease. Science 1972;176:309 - 10.
- Boldrini R, Devito R, Biselli R, Filocamo M, Bosman C. Wolman disease and cholesteryl ester storage disease diagnosed by histological and ultrastructural examination of intestinal and liver biopsy. Pathol Res Pract 2004;200:231 - 40.
- Fouchier SW, Defesche JC. Lysosomal acid lipase A and the hypercholesterolaemic phenotype. Curr Opin Lipidol 2013;24:332 - 8.
- Zhang B, Porto AF. Cholesteryl ester storage disease: protean presentations of lysosomal acid lipase deficiency. J Pediatr Gastroenterol Nutr 2013;56:682 - 5.
- Reynolds T. Cholesteryl ester storage disease: a rare and possibly treatable cause of premature vascular disease and cirrhosis. J Clin Pathol 2013;66:918 - 23.
- Saito S, Ohno K, Suzuki T, Sakuraba H. Structural bases of Wolman disease and cholesteryl ester storage disease. Mol Genet Metab 2012;105:244 - 8.
- Muntoni S, Wiebusch H, Jansen-Rust M, Rust S, Seedorf U, Schulte H, et al. Prevalence of cholesteryl ester storage disease. Arterioscler Thromb Vasc Biol 2007;27:1866 - 8.
- Lohse P, Maas S, Elleder M, Kirk JM, Besley GT, Seidel D. Compound hetero-zygosity for a Wolman mutation is frequent among patients with cholesteryl ester storage disease. J Lipid Res 2000;41:23 - 31.
- Scott SA, Liu B, Nazarenko I, Martis S, Kozlitina J, Yang Y, et al. Frequency of the cholesteryl ester storage disease common LIPA E8SJM mutation (c. 894G>A) in various racial and ethnic groups. Hepatology 2013;58:958 - 65.
- Stitziel NO, Fouchier SW, Sjouke B, Peloso GM, Moscoso AM, Auer PL, et al. Exome sequencing and directed clinical phenotyping diagnose cholesterol ester storage disease presenting as autosomal recessive hypercholesterolemia. Arterioscler Thromb Vasc Biol 2013;33:2909 - 14.
- Meikle PJ, Hopwood JJ, Clague AE, Carey WF. Prevalence of lysosomal storage disorders. J Am Med Assoc 1999;281:249 - 54.
- Valles-Ayoub Y, Esfandiarifard S, No D, Sinai P, Khokher Z, Kohan M, et al. Wolman disease (LIPA p. G87V) genotype frequency in people of Iranian-Jewish ancestry. Genet Test Mol Biomarkers 2011;15:395 - 8.
- Muntoni S, Wiebusch H, Jansen-Rust M, Rust S, Schulte H, Berger K, et al. Heterozygosity for lysosomal acid lipase E8SJM mutation and serum lipid concentrations. Nutr Metab Cardiovasc Dis 2013;23:732 - 6.
- Jeon TI, Osborne TF. SREBPs: metabolic integrators in physiology and metabolism. Trends Endocrinol Metab 2012;23:65 - 72.
- Ginsberg HN, Le NA, Short MP, Ramakrishnan R, Desnick RJ. Suppression of apolipoprotein B production during treatment of cholesteryl ester storage disease with lovastatin. Implications for regulation of apolipoprotein B synthesis. J Clin Invest 1987;80:1692 - 7.
- Quinn AG, Burton B, Deegan P, Di Rocco M, Enns GM, Guardamagna O, et al. Sustained elevations in LDL cholesterol and serum transaminases from early childhood are common in lysosomal acid lipase deficiency. Mol Genet Metab 2014;111: S89.
- Garver WS, Jelinek D, Meaney FJ, Flynn J, Pettit KM, Shepherd G, et al. The National Niemann-Pick type C1 disease database: correlation of lipid profiles, mutations, and biochemical phenotypes. J Lipid Res 2010;51:406 - 15.
- Ramirez CM, Liu B, Aqul A, Taylor AM, Repa JJ, Turley SD, et al. Quantitative role of LAL, NPC2, and NPC1 in lysosomal cholesterol processing defined by genetic and pharmacological manipulations. J Lipid Res 2011;52:688 - 98.
- Levy R, Ostlund Jr RE, Schonfeld G, Wong P, Semenkovich CF. Cholesteryl ester storage disease: complex molecular effects of chronic lovastatin therapy. J Lipid Res 1992;33:1005 - 15.
- Boadu E, Bilbey NJ, Francis GA. Cellular cholesterol substrate pools for adenosine-triphosphate cassette transporter A1-dependent high-density lipoprotein formation. Curr Opin Lipidol 2008;19:270 - 6.
- Bowden KL, Bilbey NJ, Bilawchuk LM, Boadu E, Sidhu R, Ory DS, et al. Lysosomal acid lipase deficiency impairs regulation of ABCA1 gene and formation of high density lipoproteins in cholesteryl ester storage disease. J Biol Chem 2011;286:30624 - 35.
- Beaudet AL, Ferry GD, Nichols Jr BL, Rosenberg HS. Cholesterol ester storage disease: clinical, biochemical, and pathological studies. J Pediatr 1977;90:910 - 4.
- Eto Y, Kitagawa T. Wolman’s disease with hypolipoproteinemia and acanthocytosis: clinical and biochemical observations. J Pediatr 1970;77:862 - 7.
- vom Dahl S, Harzer K, Rolfs A, Albrecht B, Niederau C, Vogt C, et al. Hep-atosplenomegalic lipidosis: what unless Gaucher? Adult cholesteryl ester storage disease (CESD) with anemia, mesenteric lipodystrophy, increased plasma chitotriosidase activity and a homozygous lysosomal acid lipase -1 exon 8 splice junction mutation. J Hepatol 1999;31:741 - 6.
- Drebber U, Andersen M, Kasper HU, Lohse P, Stolte M, Dienes HP. Severe chronic diarrhea and weight loss in cholesteryl ester storage disease: a case report. World J Gastroenterol 2005;11:2364 - 6.
- Haller W, Sharif K, Millar AJ, Brown RM, McKiernan PJ. Gallbladder dysfunction in cholesterol ester storage disease. J Pediatr Gastroenterol Nutr 2010;50:555 - 8.
- Marshall WC, Ockenden BG, Fosbrooke AS, Cumings JN. Wolman’s disease. A rare lipidosis with adrenal calcification. Arch Dis Child 1969;44:331 - 41.
- van der Graaf A, Avis HJ, Kusters DM, Vissers MN, Hutten BA, Defesche JC, et al. Molecular basis of autosomal dominant hypercholesterolemia: assessment in a large cohort of hypercholesterolemic children. Circulation 2011;123:1167 - 73.
- Pisciotta L, Fresa R, Bellocchio A, Pino E, Guido V, Cantafora A, et al. Cholesteryl Ester Storage Disease (CESD) due to novel mutations in the LIPA gene. Mol Genet Metab 2009;97:143 - 8.
- The Coronary Artery Disease (C4D) Genetics Consortium. A genome-wide association study in Europeans and South Asians identifies five new loci for coronary artery disease. Nat Genet 2011;43:339 - 44.
- The IBC 50K CAD Consortium. Large-scale gene-centric analysis identifies novel variants for coronary artery disease. PLoS Genet 2011;7: e1002260.
- Wild PS, Zeller T, Schillert A, Szymczak S, Sinning CR, Deiseroth A, et al. A genome-wide association study identifies LIPA as a susceptibility gene for coronary artery disease. Circ Cardiovasc Genet 2011;4:403 - 12.
- Wolman M, Sterk VV, Gatt S, Frenkel M. Primary familial xanthomatosis with involvement and calcification of the adrenals. Report of two more cases in siblings of a previously described infant. Pediatrics 1961;28:742 - 57.
- Freudenberg F, Bufler P, Ensenauer R, Lohse P, Koletzko S. Cholesteryl ester storage disease: an easily missed diagnosis in oligosymptomatic children. Z Gastroenterol 2013;51:1184 - 7.
- Guardamagna O, Cagliero P, Abello F. Management of inherited atherogenic dyslipidemias in children. Ther Apher Dial 2013;17:150 - 61.
- Hamilton J, Jones I, Srivastava R, Galloway P. A new method for the measurement of lysosomal acid lipase in dried blood spots using the inhibitor Lalistat 2. Clin Chim Acta 2012;413:1207 - 10.
- Mukherjee M. Human digestive and metabolic lipases - a brief review. J Mol Catal B Enzym 2003;22:369 - 76.
- Rosenbaum AI, Cosner CC, Mariani CJ, Maxfield FR, Wiest O, Helquist P. Thiadiazole carbamates: potent inhibitors of lysosomal acid lipase and potential Niemann-Pick type C disease therapeutics. J Med Chem 2010;53:5281 - 9.
- Chalasani N, Younossi Z, Lavine JE, Diehl AM, Brunt EM, Cusi K. The diagnosis and management of non-alcoholic fatty liver disease: practice guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology 2012;55:2005 - 23.
- Vajro P, Lenta S, Socha P, Dhawan A, McKiernan P, Baumann U, et al. Diagnosis of nonalcoholic fatty liver disease in children and adolescents: position paper of the ESPGHAN Hepatology Committee. J Pediatr Gastro-enterol Nutr 2012;54:700 - 13.
- Thelwall PE, Smith FE, Leavitt MC, Canty D, Hu W, Hollingsworth KG, et al. Hepatic cholesteryl ester accumulation in lysosomal acid lipase deficiency: non-invasive identification and treatment monitoring by magnetic resonance. J Hepatol 2013;59:543 - 9.
- Reiner Z. Statins in the primary prevention of cardiovascular disease. Nat Rev Cardiol 2013;10:453 - 64.
- Tarantino MD, McNamara DJ, Granstrom P, Ellefson RD, Unger EC, Udall Jr JN. Lovastatin therapy for cholesterol ester storage disease in two sisters. J Pediatr 1991;118:131 - 5.
- Tadiboyina VT, Liu DM, Miskie BA, Wang J, Hegele RA. Treatment of dyslipidemia with lovastatin and ezetimibe in an adolescent with cholesterol ester storage disease. Lipids Health Dis 2005;4:26.
- Yokoyama S, McCoy E. Long-term treatment of a homozygous cholesteryl ester storage disease with combined cholestyramine and lovastatin. J Inherit Metab Dis 1992;15:291 - 2.
- McCoy E, Yokoyama S. Treatment of cholesteryl ester storage disease with combined cholestyramine and lovastatin. Ann N Y Acad Sci 1991; 623:453 - 4.
- Leone L, Ippoliti PF, Antonicelli R. Use of simvastatin plus cholestyramine in the treatment of lysosomal acid lipase deficiency. J Pediatr 1991;119:1008 - 9.
- Abello F, Guardamagna O, Baracco V, Bonardi R. The treatment of colesteryl storage disease (CESD) by ezetimibe monotherapy. Atheroscler Suppl 2010;11:28.
- Xu M, Liu K, Swaroop M, Porter FD, Sidhu R, Firnkes S, et al. 5-Tocopherol reduces lipid accumulation in Niemann-Pick type C1 and Wolman cholesterol storage disorders. J Biol Chem 2012;287:39349 - 60.
- Ambler GK, Hoare M, Brais R, Shaw A, Butler A, Flynn P, et al. Orthotopic liver transplantation in an adult with cholesterol ester storage disease. JIMD Rep 2013;8:41 - 6.
- Grabowski GA. Therapy for lysosomal acid lipase deficiency: replacing a missing link. Hepatology 2013;58:850 - 2.
- Balwani M, Breen C, Enns GM, Deegan PB, Honzik T, Jones S, et al. Clinical effect and safety profile of recombinant human lysosomal acid lipase in patients with cholesteryl ester storage disease. Hepatology 2013;58:950 - 7.
- Whitley CB. North American Society for Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN) Annual Meeting 2013 [Oral Presentation, 11 October 2013].
- Graham I, Atar D, Borch-Johnsen K, Boysen G, Burell G, Cifkova R, et al. European guidelines on cardiovascular disease prevention in clinical practice: executive summary. Atherosclerosis 2007;194:1 - 45.
- Sloan HR, Fredrickson DS. Rare familial diseases with neutral lipid storage. In: Stanbury JB, Wyngaarden JB, Fredrickson DS, editors. The metabolic basis of inherited disease. New York: McGraw Hill Inc; 1972. p. 808.
- Yatsu FM, Hagemenas FC, Manaugh LC, Galambos T. Cholesteryl ester hydrolase activity in human symptomatic atherosclerosis. Lipids 1980;15: 1019 - 22.
Опубликовано :
ПОРАЖЕНИЯ ПЕЧЕНИ ПРИ БОЛЕЗНИ ВОЛЬМАНА У ДЕТЕЙ. Экспериментальная и клиническая гастроэнтерология. 2017;137(01):68-77
Загрузить полный текстt
-
- ОСП «Научно-исследовательский клинический институт педиатрии имени академика Ю. Е. Вельтищева» (Москва, Россия)
- ГБОУ ВПО РНИМУ им. Н. И. Пирогова (Москва, Россия)
Ключевые слова:анафилаксия,дети, пищевая аллергия
Резюме:Введение: в Российской Федерации проблема пищевой анафилаксии у детей освещается крайне редко и подобные исследования исключительно актуальны. Целью данного исследования является определение у детей особенностей этиологии и клинической картины пищевой анафилаксии, возникающей при употреблении рыбы. Материалы и методы: В исследование включено 80 детей в возрасте от 8 месяцев до 18 лет с диагнозом пищевая анафилаксия. Пациентам проводилось аллергологическое обследование, включающее определение (ImmunoCAP 100 Phadia AB, Швеция) концентрации специфических IgE в сыворотке крови к аллергенам предположительно вызвавшим анафилактические реакции. Все дети были анкетированы посредством разработанного авторами опросника, включающего вопросы относительно причин возникновения, клинических проявлений и лечения анафилаксии. Результаты: У 33,7% обследованных детей с пищевой анафилаксией имели место анафилактические реакции при употреблении рыбы. У 77,8% пациентов анафилактическая реакция на рыбу возникала однократно, У 22,2% детей имели место повторные анафилактические реакции к рассматриваемому аллергену. 3 пациента отмечали развитие анафилактических реакций уже при первом в жизни употреблении рыбы. У всех детей с анафилаксией к рыбе была выявлена сенсибилизация к данному аллергену (IgE ≥ 0,35 кUA/l). У 38,5% пациентов симптомы анафилаксии возникали при ингаляционном попадании аллергена рыбы. Частота развития анафилактических реакций при ингаляционном пути попадания аллергена рыбы в организм у детей с уровнем специфических антител к рыбе sIgE < 100 кUA/l (25%) была более чем в два раза ниже, относительно частоты развития ингаляционной гиперчувствительности к данному аллергену с уровнем сенсибилизации sIgE ≥ 100 кUA/l (54,5%). При развитии анафилактических реакций к рыбе наиболее часто выявлялись симптомы со стороны кожи/слизистых (97,5%), органов дыхательной системы (92%), сердечно-сосудистой системы (44,4%), а частота тяжелых эпизодов была достаточно высокой и составила 22%. Заключение: Более чем у 1/3 детей, страдающих пищевой анафилаксией, причиной анафилактических реакций выступает рыба. Развитие анафилаксии к рыбе возможно уже при первом в жизни ее употреблении. Определение уровня специфических IgE антител к рыбе целесообразно не только для подтверждения диагноза анафилаксии, но и для определения объема элиминационных мероприятий у данной группы пациентов.
-
- Simons F. E., Sampson H. A. Anaphylaxis epidemic: fact or fiction? J Allergy Clin Immunol. 2008; 122: 1166 - 1168.
- Esakova N. V., Treneva M. S., Okuneva T. S., Pampura A. N. Food Anaphylaxis: Reported Cases in Russian Federation Children. American Journal of Public Health Research. 2015; 3 (5): 187 - 191.
- Пампура А. Н., Конюкова Н. Г. Анафилаксия к пищевым продуктам у детей раннего возраста Российский вестник перинатологии и педиатрии. 2011; 5:76 - 84
- Muraro A., Werfel T., Hoffmann-Sommergruber K., Roberts G. et al., A. EAACI food allergy and anaphylaxis guidelines: diagnosis and management of food allergy. Allergy. 2014; 69 (8): 1008 - 1025.
- Turner P., Ng I., Kemp A. et al. Seafood allergy in children: a descriptive study. Ann. Allergy Asthma Immunol. 2011; 106 (6):494 - 501.
- Mourad A. A., Bahna S. L. Fish-allergic patients may be able to eat fish. Exprt. Rev. Clin. Immunol. 2015; 11 (3):419 - 430.
- Варламов Е., Е., Пампура А. Н., Окунева Т. С. Взаимосвязь сенсибилизации к пищевым аллергенам и тяжести атопического дерматита у детей раннего возраста. Российский Аллергологический журнал. 2008; 5: 19 - 24.
- Nwaru B. I., Hickstein L., Panesar S. S. et al. Prevalence of common food allergies in Europe: a systematic review and meta-analysis. Allergy. 2014; 69 (8): 992 - 1007.
- Huang, F., Chawla K., Järvinen K. M. et al. Anaphylaxis in a New York City pediatric emergency department: Triggers, treatments, and outcomes. J. Allergy Clin. Immunol. 2012; 129 (1): 162 - 168.
- Taylor-Black S., Wang J. The prevalence and characteristics of food allergy in urban minority children. Ann. Allergy. Asthma Immunol. 2012; 109 (6): 431 - 437.
- Федорова О. С., Огородова Л. М., Федотова М. М., Петровский Ф. И., Евдокимова Т. А., Балашева И. И. Исследование распространенности аллергии к рыбе у детей в Томской области. Российский Аллергологический журнал. 2014; 4: 39 - 44.
- Grabenhenrich L. B., Dölle S., Moneret-Vautrin A. et al. Anaphylaxis in children and adolescents: The European Anaphylaxis Registry. J. Allergy Clin. Immunol. 2016. In press
- Taylor S. L., Hefle S. L., Bindslev-Jensen C. et al. Factors affecting the determination of threshold doses for allergenic foods: how much is too much? J. Allergy Clin. Immunol. 2002; 109 (1): 24 - 30.
- Sackesen C., Adalioglu G. Hidden fish substance triggers allergy. J. Investig. Allergol. Clin. Immunol. 2003; 13 (3): 216 - 217.
- Kmet A., Unger J., Jahangir K., Kolber M. R. Fish-oil capsule ingestion: a case of recurrent anaphylaxis. Can. Fam. Physician. 2012; 58 (7): 379 - 81.
- Mejía-Rentería H. D., Viana-Tejedor A., Sánchez-Enrique C. et al. Kounis syndrome after ingestion of undercooked fish: new role of intracoronary imaging techniques. Int. J. Cardiol. 2014; 177 (2): 58 - 60.
- Leonardi S., Pecoraro R., Filippelli M. et al. Allergic reactions to foods by inhalation in children. Allergy Asthma Proc. 2014; 35 (4): 288 - 294.
Опубликовано :
КЛИНИКО-ИММУНОЛОГИЧЕСКИЕ ОСОБЕННОСТИ ДЕТЕЙ С АНАФИЛАКСИЕЙ К РЫБЕ. Экспериментальная и клиническая гастроэнтерология. 2017;137(01):78-82
Загрузить полный текст
-
- ГБОУ ВПО Санкт-Петербургский Государственный Педиатрический Университет (Санкт-Петербург, Россия)
- Северо-Западный федеральный медицинский исследовательский центр им. В. А. Алмазова Минздрава России (Санкт-Петербург, Россия)
Ключевые слова:дети,целиакия,аллергическая энтеропатия
Резюме:Данная статья описывает клинический случай целиакии у ребенка. Особенностями которого стало наличие сопутствующей патологии в виде аллергической энтеропатии, что затрудняло дифференциальную диагностику, и осложнения в виде вторичной энтеропатии. А также рассмотрена динамика пациента на фоне девятимесячной диеты. Данный случай является особенно интересным в виду растущей частоты аллергической патологии и глютен ассоциированных заболеваний.
-
- Ревнова М. О., Бельмер С. В. Целиакия у детей. Монография. Медпрактика. М. 2013;414
- Ревнова М. О., Шаповалова Н. С. Целиакия как аутоиммунное заболевание. Вопросы детской диетологии. 2015; 13 (3). 33 - 40
- Ciarán P., Kelly C. P., Julio C Bai et al. Advances in Diagnosis and Management of Celiac Disease Gastroenterology. 2015; 148 (6): 1175 - 1186
- Julio C Bai., Gino M. F., Corazza R. et al. World Gastroenterology Organisation Global Guidelines 2012
- Ludvigsson J. F., Card T. R., Kaukinen K. et al. Screening for celiac disease in the general population and in high-risk groups. United European Gastroenterology Journal. 2015; 3 (2) 106 - 120
- Новикова В. П., Абдул-заде И. Э., Гуркин Ю. А. и др. К вопросу об аутоиммунном оофорите при целиакии у подростков и взрослых. Российский иммунологический журнал. 2008; 2 (2-3) 11:236 - 237.
- Sapone A., Julio C Bai, Ciacci C. et al. Spectrum of gluten-related disorders: consensus on new nomenclature and classification BMC Medicine 2012, 10:13
- Catassi C, Julio C. Bai, Bonaz B. et al. Non-Celiac Gluten Sensitivity: The New Frontier of Gluten Related Disorders Nutrients 2013; 5, 3839 - 3853
- Elli L., Branchi F.,.Tomba C et al. Diagnosis of gluten related disorders: Celiac disease, wheat allergy and nonceliac gluten sensitivity. World J Gastroenterol. 2015; 21; 21 (23): 7110 - 7119
- Tovoli F., Masi C., Guidetti E. et al. Clinical and diagnostic aspects of gluten related disorders. World J. Clin. Cases. 2015; 3 (3): 275 - 284
Опубликовано :
ОСЛОЖНЕННАЯ ЦЕЛИАКИЯ У 4-ЛЕТНЕГО РЕБЕНКА С АЛЛЕРГИЧЕСКОЙ ЭНТЕРОПАТИЕЙ. Экспериментальная и клиническая гастроэнтерология. 2017;137(01):83-87
Загрузить полный текст
-
- ФБГУ «СЗФМИЦ им. В. А. Алмазова» (Санкт-Петербург, Россия)
- СПбГМУ им акад И. П. Павлова (Санкт-Петербург, Россия)
Ключевые слова:неонатология,недоношенные новорожденные,аллергия к белку коровьего молока,аллергический энтероколит
Резюме:В статье представлен случай аллергического энтероколита, связанного с использованием коровьего молока, у новорожденного недоношенного ребенка. Данный синдром редко встречается у недоношенных детей и характеризуется вздутием живота, срыгиваниями, примесью крови в стуле, беспокойством, лабораторно проявляется эозинофилией в общем анализе крови, в тяжелых клинических случаях на рентгенограмме органов брюшной полости можно обнаружить пневматоз кишки. Своевременная диагностика данного заболевания и дифференциальная диагностика с проявлениями некротического энтероколита определяет дальнейшую тактику лечения пациента.
-
- Баранов А. А., Намазова- Баранова Л. С. Федеральные клинические рекомендации по оказанию медицинской помощи детям с аллергией к белкам коровьего молока. 2015 г, 28с
- Koletzko S., Niggerman B., Arato A., Dias J. A., Heuschkel R., Husby S., Mearin M. L., Papadopoulou A., Ruemmele F. M., Staiano A., Schappi M. G., Vandenplas Y. Diagnostic Approach and Management of Cow’s-Milk Protein Allergy in Infants and Children: ESPGHAN GI Committee Practical Guidelines. IPGN - 2012 - Vol. 55, - P. 221 - 229.
- Food Allergy and Anaphylaxis Guidelines. EAACI. 2014, 278p
- Miyazawa T, Itahashi K, Imai T. Management of neonatal cow’s milk allergy in high-risk neonates. Pediatr Int 2009;51:544 - 7
- Morita Y., Iwakura H., Ohtsuka H., Kohno Y., Shimojo N. Milk allergy in the neonatal intensive care unit: comparison between premature and full-term neonates. Asia Pacific Allergy - 2013 - Vol. 3, - P. 35 - 41
- Maloney J., Nowak-Wegrzyn A. Educational clinical case series for pediatric allergy and immunology: allergic proctocolitis, food protein-induced enterocolitis syndrome and allergic eosinophilic gastroenteritis with protein-losing gastroenteropathy as manifestations of non-IgE-mediated cow’s milk allergy. Pediatr Allergy Immunol - 2007- Vol. 18, - P. 360 - 367.
- Srinivasan P., Brandler M., D’Soura A., Millman P., Moreau H. Allergic enterocolitis presenting as recurrent necrotizing enterocolitis in preterm neonates. Journal of Perinatology - 2010 - Vol. 30, - P. 431 - 433.
- Шабалов Н. П. Неонатология/ Н. П. Шабалов - Москва: «МЕДпресс-информ», 2004.-341 - 350 с.
- Boné J, Claver A, Guallar I, Plaza AM. Allergic proctocolitis, food-induced enterocolitis: immune mechanisms, diagnosis and treatment. Allergol Immunopathol (Madr) 2009;37:36 - 42.
- Faber MR, Rieu P, Semmekrot BA, Van Krieken JH, Tolboom JJ, Draaisma JM. Allergic colitis presenting within the first hours of premature life. Acta Paediatrica 2005; 94: 1514 - 1515
Опубликовано :
АЛЛЕРГИЧЕСКИЙ ЭНТЕРОКОЛИТ У НЕДОНОШЕННОГО РЕБЕНКА. Экспериментальная и клиническая гастроэнтерология. 2017;137(01):88-91
Загрузить полный текст
-
- ФГБОУ ДПО РМАНПО Минздрава России (Москва, Россия)
Резюме: Н. Е. Чернеховская родилась в г. Москве. Окончила школу с золотой медалью и поступила в 1-й ММИ им. И. М. Сеченова. По окончании института в 1971 г. поступила в клиническую ординатуру по хирургии на базе больницы им. С. П. Боткина, где проходила обучение под руководством профессора И. Б. Розанова. В 1973 г. Наталья Евгеньевна продолжила работу во вновь созданном эндоскопическом отделении больницы им. С. П. Боткина, где за короткое время освоила все основные методы эндоскопической диагностики и лечения, а в 1976 г. была зачислена ассистентом по эндоскопии на 1-ю кафедру хирургии ЦОЛИУв, которую возглавлял профессор И. Б. Розанов. В 1985 г. в ЦОЛИУв была создана первая в стране кафедра эндоскопии, на которой Н. Е. Чернеховская работает с момента ее основания по настоящее время. Основные научные исследования Н. Е. Чернеховской относятся к диагностике и лечению заболеваний верхних отделов желудочно-кишечного тракта и органов дыхания. Результаты многолетнего труда, ставшего делом всей профессиональной медицинской, педагогической и научной жизни Натальи Евгеньевны, нашли свое отражение в кандидатской диссертации на тему «Диагностическая и лечебная лапароскопия у больных механической желтухой» (1979 г.), докторской диссертации «Деформирующий бронхит: эндоскопические методы в комплексной диагностике и лечении» (1995 г.), а также в 35 монографиях, 11 патентах и более чем в 600 научных работах. Под научным руководством Натальи Евгеньевны защищено 26 кандидатских и 4 докторские диссертации. Наталья Евгеньевна Чернеховская - почитаемый в профессиональных и научных кругах врач, ученый, педагог, обладающий большим жизненным опытом, широким кругозором, прогрессивным мышлением и удивительной работоспособностью. Перечисление всех точек реального приложения Натальей Евгеньевной ее умений, знаний и опыта, не способно в полной мере отобразить истинный масштаб ее личности и таланта, а сочетание всех этих качеств способствуют обеспечению высокого содержательного и образовательного уровня учебных программ кафедры эндоскопии ФГБОУ ДПО РМАНПО Минздрава России, бессменным заведующим учебной частью которой она является. Благодаря своим человеческим и деловым качествам Наталья Евгеньевна пользуется заслуженным авторитетом и уважением коллег, слушателей, пациентов. Простое перечисление достижений профессора Н. Е. Чернеховской, продолжателя врачебной династии, не исчерпывает представлений о ней, как о враче, ученом, личности: Наталья Евгеньевна удивительно добрый, теплый, дружелюбный, отзывчивый человек, готовый всегда прийти на помощь. Друзья, коллеги и многочисленные ученики от души поздравляют Наталью Евгеньевну с юбилеем, желают ей доброго здоровья, долгих лет жизни, личных удач и новых достижений на профессиональном, научном и педагогическом поприщах, дальнейшей плодотворной деятельности на ниве охраны здоровья населения страны, подготовки квалифицированных медицинских и научных кадров.
Опубликовано :
70 ЛЕТ НАТАЛЬЕ ЕВГЕНЬЕВНЕ ЧЕРНЕХОВСКОЙ. Экспериментальная и клиническая гастроэнтерология. 2017;137(01):92-92
Загрузить полный текст
-
- University of Amsterdam (UvA) (Amsterdam, Netherlands)
Резюме:Disorders of the proximal digestive tract Peter Malfertheiner Lecture - Gastro Update Europe 2016 - Prague Review by Guido N. J. Tytgat Prof. Peter Malfertheiner from Germany reviewed the most salient recent achievements in the upper intestinal tract. Gastroesophageal reflux disease (GERD) continues to be one of the leading diagnoses in ambulatory care both in the USA and in Europe. Proton pump inhibitors (PPI) remain by far the first drug class for the initial therapy for symptomatic GERD, with a trend to increase the dose and the frequency of dosing. Even stronger inhibition of acid secretion is possible with a so-called potassium competitive acid blocker (p-cab) such as vonoprazan. Vonoprazan binds immediately and selectively to both active and resting pumps in the parietal cell; the slow dissociation from the pump explains the long-lasting acid inhibition. Moreover, the drug is not influenced by Cyp2C19 genotype. Vonoprazan shows impressive prolonged acid secretory inhibition, so far with few if any adverse effects (in contrast to previous p-cab attempts). It is to be expected that the spectacular Japanese results will be confirmed in the West and that the drug ultimately will become available in Europe. What the proper indications and mode of administration of this superior acid suppressant will be in clinical practice will require detailed study in view of the non-negligible consequences of prolonged profound acid suppression. The use of PPIs, even very long-term, is generally considered as rather safe. Yet clinicians should remain vigilant for possible adverse effects (magnesium,.vitamin B12 etc). Earlier studies pointed to a potentially enhanced risk of PPI-related community-acquired respiratory tract infection, but in a recent retrospective analysis of over 14 000 patients, there was no causal association between esomeprazole versus placebo in the occurrence of community-acquired respiratory tract infection and pneumonia, which is certainly reassuring. The PPI-clopidogrel controversy is fading away; indeed an updated meta-analysis was presented regarding the incidence of cardiovascular events and gastrointestinal bleeding in patients receiving clopidogrel with and without PPIs. The myocardial infarction rate and the overall mortality were indistinguishable between the 2 groups, which again is reassuring. More annoying is perhaps the relationship between PPI use and chronic kidney disease. In a study of the risk for atherosclerosis in 10.000 community participants, PPI use (which was more common in Caucasians, the obese and users of antihypertensives) was associated with chronic kidney disease, especially with twice-daily dosing. This finding contrasts with the detailed analysis of the long-term comparison of anti-reflux surgery versus prolonged PPI therapy where essentially no laboratory abnormalities were discovered between the 2 groups. One can only speculate why some participants in the atherosclerosis study were at risk for chronic kidney disease (pre-existent latent kidney disease, pharmacological interactions, confounders, etc). Anyhow, significant laboratory anomalies are not to be expected in reflux patients on PPI monotherapy. Intriguing was a recent pharmacoepidemiologic study showing an increased risk of dementia in PPI users. Obviously a prospective randomised clinical trial is mandatory to establish a direct cause and effect relationship between PPI use and incident dementia in the elderly. Such a study will be extremely difficult to carry out, but of high clinical relevance in view of the rising dementia and PPI use in the elderly, often as a gastric mucosal protectant. Several studies analysed the (major) effects of long-term PPI use on the colonic microbiota, and especially on the rising risk of lostridium difficile infection. There is a significantly lower abundance in gut commensals, and a lower microbial diversity in PPI users, with a significant increase in oral and upper gastrointestinal tract commensals together with increased numbers of enterococ, streptococ, staphylococ and potentially pathogenic Escherichia coli. The observed changes may well result from the removal of the low pH gastric barrier (the so-called acid sterilizer). Alginate / antacids such as Gaviscon double action, which particularly in the area of the acid pocket in the upper stomach are usually used as add-on therapy for insufficiently controlled or break-through symptoms during PPI therapy for reflux control. A recent large Chinese study showed that Gaviscon (2 tablets 4 x daily) as monotherapy could successfully relieve symptoms in mild to moderate GERD. It seems somewhat doubtful whether such results could be confirmed in the west and whether it would change the PPI dominance as first-line therapy for GERD. Esophageal columnar metaplasia or Barrett esophagus, present in 1-2% of the general population and some 10% of GERD patients, continues to generate major attention largely because of the 30-40% increased risk of esophageal adenocarcinoma. Remember that the majority of Barrett patients will not progress to cancer and that only some 5% of adenocarcinoma patients have been identified as Barrett carriers before cancer diagnosis. Is it possible to reduce the cancer risk? The overall risk of neoplastic progression can be reduced by some 30% with aspirin / NSAID therapy, by some 48% with statin therapy and by some 67% with PPI. Based on these data, many clinicians prescribe prolonged PPI therapy also in asymptomatic carriers of columnar metaplasia. Solid information upon which to base guidelines for endoscopic / bioptic surveillance (a hotly debated topic) do not exist. There is some consensus that surveillance of non-dysplastic Barrett, to decrease the risk of cancer death, should only be considered and targeted to high-risk groups: age > 50y, Caucasian, male gender, the obese, symptomatic. Also, the length of the Barrett segment is relevant. Of over 1.000 T1 adenocarcinomas, 56% occurred in long segment (>3cm) Barrett esophagus. The estimated annual cancer transition in long segment was 0.22%. Few would now disagree that patients with high-grade dysplasia should be amenable to preferentially endoscopic therapy (resection with radiofrequency ablation). A new American trial confirmed that patients with well established low-grade dysplasia should also be amenable to radiofrequency ablation. The annual rates of progression to high-grade dysplasia / early adenocarcinoma in that study were 6.6% in the surveillance arm compared to 0.77% in the radiofrequency arm. Eosinophilic esophagitis remains the most intriguing novel esophageal disorder. The rising frequency, at least in the West, is genuine. A large Danish study showed that the increased incidence and prevalence outpaces the changes in endoscopy and biopsy practice. The rise of the disease remains largely enigmatic. Insufficient microbial / parasitic allergen exposure early in life may well contribute to a predominance of a Th2- type immune response pattern later in life. A simplified pathophysiologic scheme is shown below. In the traditional definition, eosinophilic esophagitis does not respond to acid suppression. Yet many patients with eosinophilic inflammation do seem to respond to PPI therapy, the so-called PPI-responsive esophageal eosinophilia, leading to the concept that PPI-REE was a separate entity. However, sufficient data have been presented to show that eosinophilic esophagitis and PPI-REE are almost indistinguishable also from a genetic point of view. It would appear that in the initial and mild phases of the disease, symptoms may respond to acid inhibition. PPIs have anti-inflammatory effects, but PPI-responsiveness may gradually disappear as the fibrotic remodelling of the disease progresses. Therefore the first therapeutic approach is PPI therapy. Should PPI therapy fail, topically active corticosteroids should be tried. In a large multicenter trial budesonide effervescebt tablets (twice 1 or 2 mg) or viscous suspension (twice 2 mg) were compared versus placebo, and both showed high histological remission rates. Gastrointestinal bleeding remains a major life-threatening emergency, especially in the elderly and is of major current interest in view of the rising use of the novel non-vitamin K antagonist anticoagulants (noacs). In a large population-based cohort study, the hazard ratio of gastrointestinal bleeding with dabigatran was 2.29, with rivaroxaban 2.84, and with warfarin 2.87. In patients with atrial fibrillation, the risk of bleeding with dabigatran was less compared with warfarin, except for patients older than 75 years. This was confirmed in a meta-analysis of 23 studies comparing the risk of major gastrointestinal bleeding with non-vitamin K oral anticoagulants (noac) versus warfarin, showing that the bleeding risk in atrial fibrillation was not different between noacs and vitamin K antagonists. Fortunately the risk of dabigatran-related gastrointestinal bleeding can be reduced by gastroprotective agents as shown in a population-based study where the bleeding risk was 2.5% and was lowered to about half with gastroprotective agents. Detailed analysis of 10 randomized controlled trials regarding the use of PPI in the prevention of low-dose aspirin-associated upper gastrointestinal injury led to the following conclusions: PPIs decrease the risk of low-dose aspirin-associated upper gastrointestinal ulcers with 84% and of bleeding with 73%; for patients treated with dual anti-platelet therapy of low-dose aspirin and clopidogrel, PPIs prevent bleeding in 64% without increasing the risk of major adverse cardiovascular events. Moreover, PPIs were markedly superior to H2RAs in ulcer and bleeding prevention. Protection was also shown in a nation-wide Scandinavian study which showed that the use of PPI was associated with a decreased risk of gastrointestinal bleeding in post-myocardial infarction patients taking antithrombotics and treated with NSAIDS. The overall age-standardised incidence of gastric cancer (8.8 per 100,000) and cardiac cancer (3.3 per 100,000) remains high with 5-year survival rates of less than 25%. H. pylori infection, especially with virulent strains, remains the leading cause through pre-neoplastic remodelling of the gastric mucosa. Ideally, H. pylori should be eradicated before the development of irreversible pre-neoplastic lesions. The risk of cancer increases from gastritis, atrophic gastritis, intestinal metaplasia and dysplasia. The Olga system is increasingly used to monitor the changes in the gastric mucosa and to estimate the cancer risk. Arguments have been presented to take an additional biopsy of the angulus next to the standard antrum and corpus biopsies as this raises the detection of atrophy and intestinal metaplasia. Since the quality of the endoscopic equipment is continuously improving, there is a trend to move away from non-targeted to targeted biopsies, directed to areas of minor abnormality, only detectable with high-definition endoscopes, with or without supplementary technologies (chromo, NBI etc). The demand for high-quality equipment such as high-definition is supported by a sobering British retrospective analysis, revealing that 8.3% of patients with gastric cancer had their malignancy missed at endoscopy carried out within the 3 previous years. Screening of high-risk individuals and subjects in high-risk areas should ideally be conducted with the so-called gastropanel (measuring gastrin17, pepsinogen I, II, and ratio, and anti-H. pylori antibodies). As already stated, ideally H. pylori eradication should occur before gastric mucosal neoplastic remodelling, but even after endoscopic resection of gastric neoplasia, eradication may be indicated to prevent metachronous lesions in approximately 60%, as shown in a recent meta-analysis. There is a manifest revival of bismuth-based therapy for H. pylori eradication. The Maastricht V-2016 edition recommends for areas with high (>15%) clarithromycin resistance, bismuth quadruple or non-bismuth quadruple therapy (PPI, amoxicilline, clarithromycin, notroimidazol).In areas of high dual claqrithromycin and metronidazole resistance, bismuth quadruple therapy is the recommended first line treatment. Apparently concomitant non-bismuth quadruple therapy is superior to sequential therapy. Bismuth appears to act, not by direct interaction with urease or the urea channel in the inner bacterial membrane, but by impeding proton entry in the organism. The diminished fall in cytoplamic pH with acidification in the surrounding medium favors upregulation of the genes involved in growth, which allows augmented efficacy of the growth-dependent antimicrobials. Amoxicillin can be used instead of tetracycline in first-line bismuth quadruple therapy as shown in a large important Chinese study comparing 14 d therapy with bismuth, lanzoprazole, amoxicillin, and metronidazole (cure rates 94 and 93% for metronidsazole sensitive vs resistant) and bismuth, lanzoprazole, amoxicillin, and clarithromycin (cure rates 99 and 77% for clarithromycin sensitive vs resistant). Overall recommendations in case of eradication failure are summarised below: Novel eradication schemes have been attempted in case of eradication failure with non-bismuth quadruple therapy such as: bismuth, esomeprazole, amoxicillin, levofloxacin (cure rate 74% in highly resistant patients: amoxicillin 8%; clarithromycin 56%; metrnidazole 74%; levofloxacin 36%) bismuth quadruple; omeprazole and pylora (=bismuth subcitrate, tetracycline, metronidazole) for 10 d (cure 83% in patients with resistance to metronidazole, clarithromycin and fluoroquinolone or with multiple prior treatment failures). adding rifabutin to pantoprazol and amoxicillin or rifabutin to pantoprazol, amoxicillin, and bismuth. More intensified acid suppression with the novel p-cab vonoprazan was shown to improve the eradication rates from 76% [lanzoprazole, amoxicillin, clarithromycin] to 93% [vonoprazan, amoxicillin, clarithromycin] in over 600 gastroduodenal ulcer patients. D’Alessandro A et al. Pathological mechanisms underlying therapy of EoE. World J Gastrointest Pathophysiol 2015;6:150 Malfertheiner et al., GUT 2012 May; 61 (5):646-64; GUT 2016 subm
Опубликовано :
DISORDERS OF THE PROXIMAL DIGESTIVE TRACT Peter Malfertheiner Lecture - Gastro Update Europe 2016 - Prague. Экспериментальная и клиническая гастроэнтерология. 2017;137(01):93-95
Загрузить полный текст
-
- University of Amsterdam (UvA) (Amsterdam, Netherlands)
Резюме:Novel developments in pancreatic disorders Peter Layer Lecture - Gastro Update Europe 2016 - Prague Review by Guido N. J. Tytgat Prof Peter Layer from Germany analysed the recent novel findings with respect to pancreatic diseases. First discussed was acute pancreatitis, still a devastating entity. Excessive alcohol intake and smoking are well established causes of chronic pancreatitis; their role in the pathogenesis of acute pancreatitis is less clear. A large case-control study with over 500 patients with acute pancreatitis compared to over 10,000 matched controls. It was clearly shown that the risk of acute pancreatitis rises with rising daily alcohol intake: ~50g-3 fold; ~70g-4.2fold; ~90g-5.3 fold; >100g-6.4 fold. Also, tobacco smoking increases the risk of acute pancreatitis approximately 2 fold, as shown in a meta-analysis of 12 studies. Clinicians should therefore be aware that smoking is a potential cause of ‘idiopathic’, especially relapsing acute pancreatitis. Such patients should therefore be strongly advised to quit smoking. How smoking leads to acute pancreatitis remains poorly understood. What is also insufficiently realised in practice is that pancreatic cancer may occasionally present as acute pancreatitis. In a large American cohort with over 500,000 subjects, approximately 1 in 10 pancreatic cancers manifested first as acute pancreatitis. Most cancers became overt within 2 years post the presentation with acute pancreatitis. Whenever therefore, the cause of acute pancreatitis is not clear, meticulous EUS examination of the pancreas is indicated in order not to delay the detection of the underlying malignancy. Hypertriglyceridemia is a well established cause of acute pancreatitis. Disease severity and risk of persistent organ failure are high, and parallel the severity of hypertriglyceridemia: mild < 200; moderate < 1,000; severe > 1,000 mg / dl. It is beyond doubt that hyper triglyceridemia is strongly associated with severe and complicated acute pancreatitis, either as the sole etiology or as amplifier of other causes. The involved pathogenetic mechanisms and therapeutic possibilities are insufficiently elucidated. Most intriguing is the potential preventive role of statins in the prevention of acute pancreatitis, as analysed retrospectively in 4 million Californian subjects: acute pancreatitis risk (of any cause) was some 70% reduced in statin (simvastatin) users, especially with a dose of > 10 mg / d. As many confounders may be involved, these data beg for a prospective randomised study. How statins may be potentially preventive also needs further study. Up to now, there has been little consensus with respect to the timing of cholecystectomy after (mild) biliairy pancreatitis. In an important study, over 250 patients with mild biliairy pancreatitis [CRP < 100mg / l;opiate-free pain control; oral refeeding] were randomized to immediate surgery (within 3 d of admission) versus delayed surgery (> 25 d after discharge). There was a ~70% decrease in relapse of biliairy symptoms and pancreatitis or death within 6 months in the Group with immediate surgery during the index hospital admission. These results are quite persuasive and deserve to be followed-up in practice. Whether and when antimicrobials should be used in acute necrotising pancreatitis remains a moot and controversial point. An earlier meta-analysis showed a ~40% reduced mortality with antimicrobial therapy (betalactames, imipenem) but all studies had considerable methodological flaws and deficits. In a novel meta-analysis of 6 randomised controlled trials involving close to 400 patients with acute necrotizing pancreatitis, early antimicrobial administration led to a ~50% reduction in overall mortality and ~45% reduction in infected necrosis. Early antimicrobial therapy is probably useful in individual patients with extensive necrosis or a predicted severe disease course. Previous studies have shown that oral refeeding may start early in mild, and even more severe pancreatitis, but refeeding attempts are not always successful, especially in patients with hypertriglyceridemia or with persistently elevated enzymes (lipase > 2 times the norm). It is preferred not to force oral feeding from day one but to use recurrence of appetite as a reliable indicator for successful oral refeeding. Healing of severe acute pancreatitis may be associated with morphological and functional defects. A meta-analysis of 8 follow-up studies involving 234 patients with acute pancreatitis, revealed that 43% developed diabetes mellitus, 29% pancreatic exocrine insufficiency and 40% both sequellae. Appropriate follow-up is therefore mandatory. Alcohol consumption is a well-known and established cause of chronic pancreatitis. A recent high-quality case-control study involving over 400 patients and over 1,000 matched controls revealed an impressive alcohol dose-response risk; for daily alcohol intake of ~30, ~50, ~70, ~90, and >100 g, the risk for chronic pancreatitis rose from 2.8, 3.2, 9.2, 13 and 19.5 times respectively. In simple terms: daily alcohol consumption <20 g: no risk; moderate risk with linear increase at 20-60 g / d; rapid increase in risk beyond 60 g / d (> 2 glasses of wine; > pints of beer). Correlation between symptom pattern and severity and morphological objective alterations is often poor in gastroenterology. The same holds for chronic pancreatitis where no correlation between pancreatic morphological changes (obstruction, inflammation, pseudocysts etc.) and symptom pattern or severity is apparent. Interest in autoimmune pancreatitis remains intense. As a reminder, there are apparently 2 types: the more frequent type 1 (IgG4-associated systemic disease, often involving multiple organs) and type 2 (isolated pancreatic disease, concomitant IBD). Type 2 has been further characterized in 43 patients: 58% presented initially as relapsing acute pancreatitis; 36% presented initially as mass lesion and obstructive jaundice (mimicking cancer); 50% had associated IBD and 11% repased within 3 years after treatment. Early diagnosis is essential as the prognosis is excellent with adequate (corticosteroid) therapy. There is consensus that in principle, main duct intraductal papillary mucinous neoplasm (IPMN) should be treated surgically as cancer will develop in 1 out of 3 patients within 3 years. For branch duct IPMN, surgery is indicated for lesions larger than 3 cm, diameter of the pancreatic duct > 5 mm, presence of intramural nodules and suspicious cytology. A large study evaluated the survival in patients with main duct IPMN that could not be resected for various reasons: 5 y survival in the resected group was 74% versus 58% in the non-resected group; those older than 70 y had a significantly worse outcome as expected (comorbidities, reduced operablity etc). Statin use was also evaluated in the survival of over 200 patients resected for early-stage pancreatic cancer. Simvastatin reduced the mortality by 44% and the relapse rate by 39% if a high dose was used. It is utterly intriguing why simvastatin may improve the prognosis following curative resection of early-stage pancreatic cancer. Prospective, high-quality studies are urgently needed to consider simvastatin use as standard adjunctive anticancer therapy.
Опубликовано :
NOVEL DEVELOPMENTS IN PANCREATIC DISORDERS Peter Layer Lecture - Gastro Update Europe 2016 - Prague. Экспериментальная и клиническая гастроэнтерология. 2017;137(01):96-97
Загрузить полный текст
-
- University of Amsterdam (UvA) (Amsterdam, Netherlands)
Резюме:Gastrointestinal infections Herbert Tilg Lecture - Gastro Update Europe 2016 - Prague Review by Guido N. J. Tytgat Some recent developments in gastrointestinal infections were summarized by Prof Herbert Tilg from Austria. First discussed was the importance of the rising outbreaks of norovirus infection, the most frequent cause of foodborn illness together with Campylobacter infection. Norovirus, a calicivirus, has a worldwide distribution (incubation period is 24-48 h), with symptoms lasting ~48-72 hours and viral shedding in stool continuing for 2-3 weeks. Viral identification is mandatory especially in an outbreak setting with nucleic acid based testing (RT-PCR) or immuno-assay. Vomiting is a key clinical symptom. Particular attention is required when alarm symptoms develop, such as dehydration, enteral bleeding, weight loss, severe abdominal pain, and if symptoms last longer than a week, especially in the elderly or in immunosuppressed people. End 2014, a more virulent genotype variant appeared, which is more capable of immune evasion, causing severe gastroenteritis and often necessitating hospitalisation. It is unfortunate that no antiviral therapy is available; vaccines are under development. Hand wash with soap and water for 30 seconds removes the virus from finger pads in contrast to washing with propanol-based hand desinfectant, which shows little viral reduction. Campylobacter infection, the most common cause of bacterial diarrhea is largely a foodborn disease. Campylobacter inhabits the intestinal tract of many animals, most notably poultry. The incubation period lasts ~3 days. The disease presents with fever, followed by abdominal cramps and diarrhea. Late complications are reactive arthritis and Guillain Barre syndrome. Therapy focuses on rehydration; antibiotics should be limited to severe disease (ciprofloxacin, azithromycin). Most intriguing, based on a meta-analysis, is the finding that Campylobacter infection increases the risk of IBD, in contrast to H. Pylori infection which seems negatively associated with IBD. This observation begs for understanding. Clostridium difficile colonizes the human intestinal tract after the normal gut flora has been altered by antimicrobial therapy. The spectrum of clinical presentation is highly variable. Life threatening disease, including fulminant colitis, is possible. Testing for toxin is recommended for symptomatic patients with nosocomial infection. In a large European multicenter (482 hospitals), prospective bi-annual point-prevalence study of Clostridium difficile infection in hospitalised patients with diarrhea, it was shown that - absence of clinical suspicion and suboptimal laboratory diagnostic methods were responsible - 40,000 European inpatients per year with Clostridium difficile infection were not diagnosed properly. Note that PCR testing will lead to overdiagnosis of Clostridium difficile infection; measuring the presence of toxin is essential for adequate diagnosis. All Clostridium difficile infection-related complications and deaths occur only in toxin-positive patients. Patients with a positive OPCR, but with a negative toxin assay, had similar outcomes as patients without Clostridium difficile infection. It is also wise to remember that there is a high rate of alternative diagnoses in patients refered for presumed Clostridium difficile infection; indeed up to 25% of such patients have a non-Clostridium difficile diagnosis, mainly IBD and IBS. Morbidity and mortality of Clostridium difficile infection in postoperative patients is alarmingly high. Almost 500,000 post-sugical patients in well over 100 American hospitals were analysed. The Clostridium difficile infection rate was 0.4% per year. Risk factors were: age, frequently hospitalisation, complex surgery, and increased antimicrobial use. Postoperative morbidity was higher and 30 day mortality was 5.3% compaired to 1.0% in non-infected patients. Therapeutic recommendations may be summarized as follows: moderately severe: oral metronidazole (3 x 500 mg) or vancomycin (4 x 125 mg) for 2 weeks. severe disease: iv metronidazole: oral / nasogatral vancomycin (4 x 500 mg) or fidaxomicin (2 x 200 mg) for 2 weeks. complicated disease: see above, plus fecal microbiota transplantation (FMT). The initial spectacular results of TMT, at first infused via the proximal intestine, have been confirmed - also infused via the colon, and in patients with very severe and complicated infection, and further in patients with toxic megacolon. The FMT technology is constantly evolving; frozen microbiota seems equally efficacious as fresh stool enemas. Microbiota suspension as enema in ready-to-use format seems also safe and effective. Finally, studies are ongoing to find out if a small molecule ebselen (an anti-oxidant and antivirulence agent), targeting the cystein protein domain of toxin B, can be used clinically to control the disease. The deleterious effects of continuous PPI therapy in recurrent Clostridium difficile infection is well established. In a recent retrospective cohort study involving some 750 patients with Clostridium difficile infection, PPIs were used in 61% (of whom only about half had an evidence-based indication!). Almost none of the PPI users stopped the drug despite the proven risk. PPI use decreases the bacterial richness and results in profound microbiome changes, affecting 20% of the bacteria. Oral / pharyngeal bacteria and potential pathogenic bacteria (enterococ, streptococ, staphylococ, micrococ, etc.) increase. Some investigators even claim that PPI induce more bacterial alterations than use of antimicrobials. Exploring the role of the gut microbiome in many diverse diseases continues, also with respect to the gut-brain interaction. As an example: evidence is increasing supporting the role of the indiginous bacteria from the gut microbioma in the regulation of serotonin biosynthesis and metabolism, impacting on gastrointestinal motility, secretion, and hemostasis. Altering the microbiota may well improve 5-hydroxy triptamine-related disease symptoms such as IBS, but also other conditions. Obviously there is more to come.
Опубликовано :
GASTROINTESTINAL INFECTIONS Herbert Tilg Lecture - Gastro Update Europe 2016 - Prague.Экспериментальная и клиническая гастроэнтерология 2017;137(01):98-98
Загрузить полный текст
-
- University of Amsterdam (UvA) (Amsterdam, Netherlands)
Резюме:Developments in digestive endoscopy Andrea May, Marco Bruno and Bjorn Rembacken Lectures - Gastro Update Europe 2016 - Prague Review by Guido N. J. Tytgat Prof Andrea May from Germany covered endoscopic achievements in the upper gastrointestinal tract. There is no global consensus on the need and the characteristics of surveillance of patients with esophageal columnar metaplasia (Barrett). Most would agree that surveillance is only clinically indicated when the neoplastic risk is truly enhanced. Based on a large cohort of over 1,000 esophageal early adenocarcinoma, cancer was more common in long segment Barrett (> 3 cm) (56%) compared to short segment (< 3 cm) metaplasia (24%). The authors conclude that the cancer incidence per 100,000 population is 3.3 for long segment compared 1.4 for short segment. Based on these findings, it would appear that Barrett length should be integrated in the surveillance advice: every 2-3 y for long segment, every 5 y for short segment. We are again reminded that surveillance is a difficult procedure, requiring optimal equipment, optimal dedication, and expertise for adequate detection of neoplasia. In a prospective surveillance study of routine clinical practice of 121 patients with Barrett neoplasia, only one third of the neoplastic lesions were correctly identified at endoscopy. The other two thirds were initially considered as non-suspicious aberrations; particularly type IIb (flat, non-elevated) were prone to misinterpretation. Because detection and proper identification of flat neoplasia is difficult, it is probably still wise to take 4-quadrant non-targeted biopsies during the index endoscopy to diminish the risk of missing neoplastic changes. Peroral endoscopic myotomy (POEM) was added to pneumodilation and laparoscopic Heller myotomy for the treatment of achalasia. The long-term results of the large multicenter prospective trial comparing pneumodilation to laparascopic myotomy have become available. In that study, re-pneumodilation was allowed twice if this therapy was initially successful and if symptoms recurred beyond 2 years after the first pneumodilation; treatment failure was decided if symptoms recurred sooner. Respective per protocol 5 years success was 91 versus 82%, and intention-to-treat success was 82 versus 84% for pneumodilation and laparoscopic myotomy; perforation occurred in 5% after pneumodilation and mucosal injury occurred in 12% after myotomy. This study therefore illustrates that both techniques are comparable from a clinical point of view. The choice of therapy should at large be based on local expertise. Certainly in the younger patients (< 40 y) myotomy by an experienced surgeon deserves to be considered. While the technique of POEM continues to improve, follow-up data from the intial studies are becoming available. 80 patients from a multicenter study were followed-up for 2-3 years. The initial success rate of 96% dropped to 78% beyond 2 years of follow-up. Initial failure (4%) and disease recurrence (18%) occurred mainly during the learning phase of the procedure. Endoscopic reflux esophagitis was diagnosed in 40% (!) of the patients, usually requiring prolonged PPI therapy. POEM is certainly an attractive novel procedure but may not be superior to the other treatment modalities, and cannot yet be recommended as the new standard therapy of choice. Endoscopic hemostasis with hemostatic powder (such as hemospray etc) continues to be explored particularly with respect to the proper indications (diffuse bleeding, difficult bleeding areas to reach, failure of other hemostatic modalities, etc. In a study with 40 patients with upper-intestinal, non-variceal bleeding, initial hemostasis was obtained with hemospray in 95% but bleeding recurred in 30%. Interestingly, no hemostatic powder was endoscopically detectable after 24 hours. For the time being, hemostatic powder should be considered as a reserve method together with the standard endoscopic hemostatic modalities: injection of saline / epinephrine; mechanical clipping and ligation; thermal electrocoagulation. The number of patients on anticoagulants (vitamin-K antagonists, such as warfarin or the novel oral anticoagulants, such as dabigatran) that need an endoscopic procedure is increasing. Low risk procedures are upper and lower endoscopy + biopsy, biliary or pancreatic stenting, and diagnostic EUS. High risk procedures include: polypectomy, sphincterotomy, EUS with fine needle aspiration, PEG, variceal banding and stricture dilation. To prevent peri-operative bleeding, inpatients with atrial fibrillation, warfarin is usually stopped 5 days before the procedure and low-molecular weight heparin is given as peri-operative bridging. Warfarin can be resumed within 24 hours after the procedure. In a large study with almost 2,000 patients with atrial fibrillation, heparin was compared with placebo as briding in patients with a mean CSAD2 score of 2, 3; arterial thromboembolism occurred in 0.3 versus 0.4% but major bleeding in 3.2 versus 1.3% respectively in the heparin versus the placebo group. The authors conclude that for low risk interventions and a CHAD2 score =< 2, no bridging with heparin is required and warfarin can be resumed within 2 hours after the procedure at the usual dose. Currently, the CHA2DS2-VASc scoring system is often used. Following points are given: congestive heart failure 1, hypertension 1, age =>75 y 2, diabetes 1, stroke 2, vascular disease 1, age 65-74 1, female gender 1. Interest in full (transmural) thickness resection of localised mural lesions throughout the gastrointestinal tract is rising, and dedicated full thickness resection devices have recently been described. Obviously such technology should be in the hand of highly experienced endoscopists, in a center with full expertise in endoscopic emergencies, but the expectation is that such endoscopic approaches will expand. The wall defect is usually closed before transmural transection, with a large over-the-scope (OTC) clip. An alternative is to suture the defect with a suturing device (over-stich; plicator; Gerdx etc). Balloon-assisted endoscopy is increasingly performed in patients with Crohn disease. In a retrospective analysis of almost 30,000 patients examined with balloon-assisted endoscopy, the overall perforation rate was 0.1%, but the risk increased 2.5 fold in Crohn, 3 fold in steroid users and 9 fold in the latter combination. Utmost attention is therefore mandatory in the presence of ulcerated lesions and concomitant steroid therapy. A rising alternative to endoscopy is dedicated MRI enterography for primary diagnosis but also for monitoring therapy. There is even some hope that in the future, MRI-based differentiation between inflammation and fibrosis will be possible and quantifiable, which will have major impact in the choice of therapy. Prof Marco Bruno from the Netherlands covered the recent findings of clinical relevance in the biliopancreatic area with ERCP and EUS. First discussed was a landmark study regarding the role of endoscopic sphincterotomy for suspected sphincter of Oddi dysfunction. These are patients with pain after cholecystectomy without significant abnormalities on imaging or laboratory studies. Sphincterotomy was randomly compared to sham, and those randomized to sphincterotomy and had an elevated pancreatic sphincter pressure were rerandomized to biliary only, or biliary and pancreatic sphincterotomy. Over 200 patients were included. To make the story short, the results were negative! The lesson for us clinicians is that we should be utterly reluctant to embark on risky sphicterotomy for a pain syndrome which is poorly understood. Further discussed was the role of endoscopic sphincterotomy for suspected sphincter of Oddi dysfunction, which is commonly performed in the USA. In a landmark multicenter American sham-controlled randomized trial involving over 200 patients with pain after cholecystectomy, without significant abnormalities on imaging or laboratory studies and without prior phincter treatment or pancreatitis, sphincterotomy was compared to sham therapy with follow-up blinded lasted for 1 year. After ERCP patients were randomized irrespective of sphincter manometry findings. Those randomized to sphincterotomy with elevated pancreatic sphincter pressure were randomized again to biliary or to both biliary and pancreatc sphincterotimy. The outcome was essentially negative; sphincterotomy (either biliary or combined biliary and pancreatic) was no better than sham placebo in relieving symptoms. Physicians should therefore be utterly reluctant to carry out a (risky) sphincterotomy if in the absence of imaging or lab abnormalities. Already in a somewhat older study, it was shown that rectal NSAIDs reduce the incidence of post-ERCP pancreatitis, which occurred in 9% of the indomethacine group, compared to 17% in the placebo group. Based on such findings, it is usually recommended to administer rectally 100 mg indomethacine or diclofenac before or after ERCP, especially in patients with an elevated baseline risk [suspected sphincter of Oddi dysfunction; prior pancreatitis; precut sphincterotomy; > 8 cannulation attempts; sphincter dilation; ampullectomy] or in patients with 2 or more minor criteria [age > 50 y; female gender; prior recurrent pancreatitis; > 3 contrast injections in the pancreatic duct; high pressure acinarization; duct cytologic sampling]. Perhaps these recommendations for rectal NSAIDs may not be as straight forward as initially thought because of the findings in a large general practice study (with ~70% at average post-ERCP pancreatitis risk) comparing 100 mg rectal indomethacine versus placebo suppository. The study did not show protection against pancreatitis, defined by new upper abdominal pain, lipase > 3 fold the upper normal level, and need for hospitalization. Puting all information together (including some recent positive studies), it is probably wise to still continue to use rectal NSAIDs in clinical practice. By the way, parenteral administration of NSAIDs has not been shown to be effective as pancreatitic prophylaxis in the past for unknown reasons. It is widely accepted that palliative drainage of malignant common bile duct obstruction should be first attempted endoscopically. Initial insertion of a 10 Fr plastic stent is recommended if the diagnosis of malignancy is not established or if expected survival is < 4 m. No drug prescription is recommended to prolong stent patency. In patients with an established diagnosis of malignancy, initial insertion of a 10 mm diameter self expanding metal stent is recommended if expected survival is > 4 m or whenever the cost of such a stent is less than half the ERCP cost. A recent study with over 200 patients compared stent patency for plastic stents (172 d), uncovered (288 d) and partially covered self-expanding metal stents (299 d). Total costs per patient at the end of the follow-up period did not differ betwen plastic stents and metal stents. Even in patients with < 3 m survival or metastatic disease, costs did not differ. Thus in the palliation of extrahepatic biliary obstruction, self expanding metal stents have a longer functional time and total costs do not differ significantly with stent type. The standard endoscopic therapy for choledocholithiasis is endoscopic sphincterotomy and basket or balloon facilitated stone extraction. Complimentary techniques for removal of large or multiple stones are mechanical lithotripsie, electrohydraulic lithotripsy, cholangioscopy with (Holmium) laser lithotripsy or extracorporeal shockwase lithotripsy. To find out if it is possible to extract large (>15 mm) or multiple (>3) stones after widening the sphincterotomy opening with a large balloon, a comparative study was performed in 70 patients comparing spincterotomy with or without balloon dilation. Complete stone removal was achieved overall in respectively 100 vs 89%; in the first session in 88 vs 56%; pancreatitis occurred in 6 vs 23%; hemorhage in 3 vs 6%; there were no perforations. Papillary large balloon dilation, with or without endoscopic sphincterotomy was retrospectively analysed in 2 other studies and revealed similar rates of large / multiple stone removal (100 vs 98%) and adverse event rates (4 vs 7%). Based on these data, American guidelines state that papillary large-balloon dilation can be used as the initial method when large common bile duct stones have been identified. If retrograde cannulation of the biliary tree fails in case of distal malignant obstruction, percutaneous transhepathic cholangiography is often attempted. The latter technique may lead to complications (bleeding, bile leak, sepsis, peritonitis) and may cause mortality (0.6-5.6%). Novel is the possibility of EUS guided transmural drainage, preferably using an all-in-one device for puncture and deployment of a partially covered metal stent or increasingly, a lumen-apposing (diabolo-type) stent. A multicenter Korean study compared EUS-guided internal versus percutaneous drainage for unresectable malignant distal biliary obstruction and inaccessible papilla. Respective technical success was 94 vs 97%, functional success was 88 vs 87%, adverse events 9 vs 31%, reintervention rate 25 vs 55%. Stent patency and overall survival were comparable. It would appear that EUS-guided internal biliary drainage may well become the therapy of choice in the future now that stent design and equipment continues to improve. Conflicting data have been reported regarding the clinical impact of on-site cytopathology evaluation during EUS-guided fine needle aspiration of pancratic masses. Observational studies have suggested that the absence of on-site cytopathology is associated with a 10-15% reduction in definite diagnosis and number of adequate specimens. Because a randomized controlled trial, comparing the impact of on-site cytopathology on the diagnostic yield and overall accuracy is lacking, a large American trial was conducted involving 240 patients. Respectively with versus without on-site cytopathology revealed a median number of needle passes of 4 vs 7, inadequate specimens of 10 vs 13% and overall accuracy of 88 vs 89%. It would therefore appear that in high volume centers there is no difference in the diagnostic yield of malignancy, accuracy, procedure time and costs between patients with pancreatic masses undergoing EUS-fine needle aspiration with or without on-site cytopathology. An obvious alternative to all this would be that the endoscopist of the future obtains some basic training in cytology slide production and evaluation, but whether this is realistic remains to be seen. Prof Bjorn Rembacken (UK) analysed endoscopy in the lower gastrointestinal tract. He first discussed the important issue of bowel cleansing. Most difficult to clean are the elderly, cirrhotics, constipated and obese patients. Adding lubiprostone to the polyethylene glycol (PEG) solution does not help. A split-dose regimen gives overall better results than the day-before cleansing, but same day cleansing is even better than splitting over 2 days. The better the cleansing result, the more sessile serrated lesions and advanced adenomas are detected, and the lesser flat lesions are missed. The higher the experience, the higher the cecal intubation rate (usually somewhat lower in women and the elderly). Cap-assisted colonoscopy has been shown to improve the adenoma / polyp detection rate, especially in the right colon. Prolonging the withdrawal / obervation time beyond 6 months increases the polyp detection rate but also decreases the risk of interval cancer occurring after the colonoscopy. Using a spasmolytic (often mebeverine) during the procedure may marginally improve the procedure. Endoscopic retrovertion, not only in the rectum but also in the right colon enhances the adenoma detection rate. Water infusion in a difficult sigmoid reduces pain and improves the adenoma detection rate, but not the cecal intubation rate. The presence of a large, flat, dysplastic polyp in the left colon points to a higher risk of polypoid lesions in the proximal colon, stressing the need for standard meticulous pan-colonoscopy. Small polyps can be removed by cold-snaring or with a large caliber foreceps. Larger lesions, not suitable for snare polypectomy, are increasingly removed by endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD). A meta-analysis of EMR versus ESD, involving well over 2,000 polyps, showed following respective results: perforation 1.4 vs 5.7%; delayed bleeding 3.5 vs 2.0%; procedure duration 30 vs 66-108 m. Of the several (ESGE, ACG) guidelines that were discussed only a few items will be covered: regarding bowel cleansing, avoid sodium phosphate and magnesium citrate preparations in the elderly, or patients with renal disease, or those taking medications that alter renal blood flow or electrolyte excretion. Avoid metoclopramide. Offer a repeat colonoscopy within 1 year in patients with inadequate preparation. If small bowel bleeding persists, the diagnostic work-up should include a repeated upper and lower endoscopy, capsule endoscopy, balloon-enteroscopy, CT or MR enterography as appropriate. Intra-operative endoscopy should be available at the time of surgery. Patients with aortic stenosis and angioectasia (Heyde syndrome) and ongoing bleeding should undergo aortic valve replacement. The American guidelines on surveillance after colorectal cancer surgery were also covered. For stage I cancer and risk factors:.CEA twice / y / 5 y;.colonoscopy after 1 y and then every 3-5 y;.5 yearly CR or MRI For stage II to III cancer:.CEA twice yearly for 5 y;.colonoscopy after 1 y and then every 3-5 y;.5 yearly CT or MRI. For stage IV metastatic disease;.CEA twice yearly for 5 y;.colonoscopy after 1 y and then every 3-5 y;.5 yearly CT or MRI.
Опубликовано :
DEVELOPMENTS IN DIGESTIVE ENDOSCOPY 99 Andrea May, Marco Bruno and Bjorn Rembacken Lectures - Gastro Update Europe 2016 - Prague. Экспериментальная и клиническая гастроэнтерология. 2017;137(01):99-101
Загрузить полный текст