")
")
-
- ФГБУ «Северо-западный федеральный медицинский исследовательский центр им. В. А. Алмазова» Минздрава России (Санкт-Петербург, Россия)
Ключевые слова:Ожирение,Бариатрическая хирургия,Внутрижелудочный баллон,Сахарный диабет,Ремиссия диабета 2 типа,ИМТ
Резюме:Цель: Ожирение представляет собой одну из наиболее насущных проблем современной медицины, являясь не только самостоятельной причиной повышения инвалидизации и смертности, но и основой для развития метаболического синдрома с его многочисленными проявлениями и сахарного диабета 2 типа. Между тем, попытки снижения веса при помощи гипокалорийных диет, фармакотерапии и изменений в образе жизни имеют ограниченную эффективность и редко дают стойкий результат. Малоинвазивные методы, такие как баллонирование желудка, эффективны лишь у части больных, а большие хирургические вмешательства имеют высокую эффективность у большинства пациентов с ожирением, но требуют пожизненных ограничений и врачебного наблюдения. Таким образом для создания эффективного алгоритма выбора лечения метаболического синдрома, требуется идентификация предикторов ответа на каждый из указанных методов лечения, что и является целью данной работы. Материалы и методы: Изучение и анализ литературы по исследованиям зарубежных авторов. Результаты: В качестве предикторов снижения веса при установке ВЖБ можно рассматривать женский пол, исходно более низкий уровнь ИМТ, отсутствие компульсивного переедания («binge eating»), при больших хирургических вмешательствах - ИМТ, уровень С-пептида и продолжительность СД2. Выводы: Суммируя результаты многочисленных исследований, к предикторам, имеющим хорошую доказательную базу в отношении снижения массы тела у пациентов с сахарным диабетом, относятся исходный ИМТ и пол. Достаточно хорошо изученными факторами компенсации гликемии на фоне лечения являются сохранная функция бета-клеток, которую эффективно отражает уровень С-пептида и сопутствующая сахароснижающая терапия. Дальнейшего изучения требуют возрастные характеристики, уровень орексигенных и анорексигенных гормонов, психо-социальные особенности пациентов, исходный уровень компенсации гликемии.
-
- CDC. National Diabetes Statistics Report, 2014. Available at: http://www.cdc.gov/diabetes/statistics/comp/fig7_overweight.htm. Last accessed September 2015.
- Calvera MA, de Aldrade M, Mesas AE, et al. W. J. Obes. 2015 Feb; 31 (2): 244-253 Is Obesity Predictive of Cardivascular disfunction independent of Cardiovascular Risk Factors?
- Williamson, DE. Descriptive epidemioiogy of body weight and body weight change in U.S. adults. Annals of lnternal Medicine, 1993; 119: 646-649.
- Laville M, Andreelli F. Mechanisms for weight gain during blood glucose normalization. Diabetes&Metabolism. 2000; 26(3): 42-5.
- Gregg EW, Chen H, Wagenknecht LE, Clark JM, Delahanty LM, Bantle J et al. Association of an intensive. lifestyle intervention with remission of type 2 diabetes. Journal of the American Medical Association. 2012;308(23):2489-96. doi: 10.1001/jama.2012.67929.
- Yanovski SZ, Yanovski JA. Long-term drug treatment for obesity: a systematic and clinical review. Journal of the American Medical Association. 2014;311(1):74-86. doi: 10.1001/jama.2013.281361.
- Hermansen K, Mortensen LS. Bodyweight changes associated with antihyperglycaemic agents in type 2 diabetes mellitus. Drug Safety 2007;30(12):1127-1142.
- UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998; 352(9131):837-53.
- Inzucchi SE. Oral antihyperglycemic therapy for type 2 diabetes: scientific review. Journal of the American Medical Association. 2002;287(3):360-372. doi:10.1001/jama.287.3.360.
- Ramhamadany EM, Fowler J, Baird IM. Effect of the gastric balloon versus sham procedure on weight loss in obese subjects. Gut. 1989;30(8):1054-7.
- Gómez V, Woodman G, Abu Dayyeh BK. Delayed gastric emptying as a proposed mechanism of action during intragastric balloon therapy: Results of a prospective study. Obesity (Silver Spring). 2016;24(9):1849-53. doi: 10.1002/oby.21555.
- Genco A, Roberta M, Massimiliano C, Emanuele S, Giovanni C, Adriano R. Endoscopic treatment: intragastric balloon. In: Lucchese M & Scopinaro N (Eds.). Minimally invasive bariatric and metabolic surgery. Springer International Publishing; 2015. p. 145-152.
- Imaz I, Martínez-Cervell C, García-Alvarez EE, Sendra-Gutiérrez JM, González-Enríquez J. Safety and effectiveness of the intragastric balloon for obesity. A meta-analysis. Obesity Surgery. 2008; 18(7):841-6. doi: 10.1007/s11695-007-9331-8.
- Mazure RA, Salgado G, Villarreal P, Cobo B, Valencia A, Culebras JM. Intragastric balloon and multidisciplinary team. Nutricion Hospitalaria. 2009;24(3):282-7.
- Kotzampassi K, Grosomanidis V, Papakostas P, Penna S, Eleftheriadis E. 500 intragastric balloons: what happens 5 years thereafter? Obesity Surgery. 2012;22(6):896-903. doi: 10.1007/s11695-012-0607-2.
- Forlano R, Ippolito AM, Iacobellis A, Merla A, Valvano MR, Niro G et al. Effect of the BioEnterics intragastric balloon on weight, insulin resistance, and liver steatosis in obese patients. Gastrointestinal Endoscopy. 2010;71(6):927-33. doi: 10.1016/j.gie.2009.06.036.
- Mui WL, Ng EK, Tsung BY, Lam CH, Yung MY. Impact on obesity-related illnesses and quality of life following intragastric balloon. Obesity Surgery. 2010;20:1128-1132. doi: 10.1007/s11695-008-9766-6.
- Genco A, López-Nava G, Wahlen C, Maselli R, Cipriano M, Sanchez MM et al. Multi-centre European experience with intragastric balloon in overweight populations: 13 years of experience. Obesity Surgery. 2013;23(4):515-21. doi: 10.1007/s11695-012-0829-3.
- Mitura K, Garnysz K. In search of the ideal patient for the intragastric balloon - short- and long-term results in 70 obese patients. Videosurgery and Other Miniinvasive Techniques. 2016;10(4):541-7. doi: 10.5114/wiitm.2015.55748.
- Kotzampassi K, Shrewsbury AD, Papakostas P, Penna S, Tsaousi GG, Grosomanidis V. Looking into the profile of those who succeed in losing weight with an intragastric balloon. Journal of laparoendoscopic & advanced surgical techniques. Part A. 2014;24(5):295-301. doi: 10.1089/lap.2013.0439.
- Martinis Fernandes FA Jr, Carvalho GL, Lima DL, Rao P, Shadduck PP, Montandon ID et al. Intragastric Balloon for Overweight Patients. Journal of the Society of Laparoendoscopic Surgeons.2016; 20(1). pii: e2015.00107. doi: 10.4293/JSLS.2015.00107.
- Tai CM, Lin HY, Yen YC, Huang CK, Hsu WL, Huang YW et al. Effectiveness of intragastric balloon treatment for obese patients: one-year follow-up after balloon removal. Obesity Surgery. 2013;23(12):2068-74. doi: 10.1007/s11695-013-1027-7.
- Madeira E, Madeira M, Guedes EP, Mafort TT, Neto LV, de Oliveira Moreira R et al. Assessment of predictive response factors to intragastric balloon therapy for the treatment of obesity. Journal of laparoendoscopic & advanced surgical techniques. Part A. 2016;26(3):168-73. doi: 10.1089/lap.2015.0305.
- Dogan UB, Gumurdulu Y, Akin MS, Yalaki S. Five percent weight lost in the first month of intragastric balloon treat-ment may be a predictor for long-term weight aintenance. Obesity Surgery. 2013;23(7):892-6. doi: 10.1007/s11695-013-0876-4.
- Ihiiya T, Nakazato M, Mizuta M et al. Plasma ghrelin levels in lean and obese humans and the effect of glucose on ghrelin secretion. J Clin Endocrinol Metab 2002; 87: 240-244.
- Mion F, Napoléon B, Roman S, Malvoisin E, Trepo F, Pujol B et al. Effects of intragastric balloon on gastric emptying and plasma ghrelin levels in non-morbid obese patients. Obesity Surgery. 2005;15(4):510-516. doi: 10.1381/0960892053723411
- Martinez-Brocca MA, Belda O, Parejo J, Jimenez L, del Valle A, Pereira JL et al. Intragastric balloon-induced satiety is not mediated by modification in fasting or postprandial plasma ghrelin levels in morbid obesity. Obesity Surgery. 2007;17(5):649-57.
- Nikolic M, Boban M, Ljubicic N, Supanc V, Mirosevic G, Pezo Nikolic B et al. Morbidly obese are ghrelin and leptin hyporesponders with lesser intragastric balloon treatment efficiency: ghrelin and leptin changes in relation to obesity treatment. Obesity Surgery. 2011;21(10):1597-604. doi: 10.1007/s11695-011-0414-1.
- Fuller NR, Lau NS, Denyer G, Caterson ID. An intragastric balloon produces large weight losses in the absence of a change in ghrelin or peptide YY. Clinical Obesity. 2013;3(6):172-9. doi: 10.1111/cob.12030.
- Bužga M, Evžen M, Pavel K, Tomáš K, Vladislava Z, Pavel Z et al. Effects of the intragastric balloon MedSil on weight loss, fat tissue, lipid metabolism, and hormones involved in energy balance. Obesity Surgery. 2014;24(6):909-15. doi: 10.1007/s11695-014-1191-4.
- Mathus-Vliegen EM, Eichenberger RI. Fasting and meal-suppressed ghrelin levels before and after intragastric balloons and balloon-induced weight loss. Obesity Surgery. 2014;24(1):85-94. doi: 10.1007/s11695-013-1053-5.
- Konopko-Zubrzycka M, Baniukiewicz A, Wróblewski E, Kowalska I, Zarzycki W, Górska M et al. The effect of intragastric balloon on ghrelin, leptin and adiponectin levels in patients with morbid obesity. Journal Of Clinical Endocrinology And Metabolism. 2009;94(5):1644-9. doi: 10.1210/jc.2008-1083.
- Crujeiras AB, Goyenechea E, Abete I, Lage M, Carreira MC, Martínez JA et al. Weight regain after a diet-induced loss is predicted by higher baseline leptin and lower ghrelin plasma levels. Journal Of Clinical Endocrinology And Metabolism. 2010;95(11):5037-44. doi: 10.1210/jc.2009-2566.
- Williams DL, Baskin DG, Schwartz MW. Leptin regulation of the anorexic response to glucagon-like peptide-1 receptor stimulation. Diabetes. 2006;55(12):3387-93. doi: 10.2337/db06-0558.
- Bacha F, Saad R, Gungor N, Arslanian SA. Adiponectin in youth, relationship to visceral adiposity, insulin sensitivity, and beta-cell function. Diabetes Care. 2004;27(2):547-52.
- Fu Y, Luo N, Klein RL, Garvey WT. Adiponectin promotes adipocyte differentiation, insulin sensitivity, and lipid accumulation. Journal of Lipid Research. 2005;46(7):1369-79. doi: 10.1194/jlr.M400373-JLR 200.
- Mathus-Vliegen EM, de Groot GH. Fasting and meal-induced CCK and PP secretion following intragastric balloon treatment for obesity. Obesity Surgery. 2013;23(5):622-33. doi: 10.1007/s11695-012-0834-6.
- Fuller NR, Lau NS, Denyer G, Caterson ID. An intragastric balloon produces large weight losses in the absence of a change in ghrelin or peptide YY. Clinical Obesity. 2013;3(6):172-9. doi: 10.1111/cob.12030
- Cugini P, Cilli M, Salandri A, Ceccotti P, Di MA, Rodio A et al. Anxiety, depression, hunger and body composition: III. Their relationships in obese patients. Eating And Weight Disorders. 1999;4(3):115-20.
- Hillman JB, Dorn LD, Huang B. Association of anxiety and depressive symptoms and adiposity among adolescent females using dual energy X-ray absorptiometry. Clinical Pediatrics (Phila). 2010;49:671-7.
- Guedes EP, Madeira E, Mafort TT, Madeira M, Moreira RO, Mendonça MC et al. Body composition and depressive/anxiety symptoms in overweight and obese individuals with metabolic syndrome. Diabetology & Metabolic Syndrome. 2013. 5(1):82. doi: 10.1186/1758-5996-5-82.
- Puglisi F, Antonucci N, Capuano P, Zavoianni L, Lobascio P, Martines G et al. Intragastric balloon and binge eating. Obesity Surgery. 2007;17(4):504-9. doi: 10.1007/s11695-007-9088-0.
- Dumonceau JM. Evidence-based review of the Bioenterics intragastric balloon for weight loss. Obesity Surgery. 2008;18(12):1611-7. doi: 10.1007/s11695-008-9593-9.
- Deliopoulou K, Konsta A, Penna S, Papakostas P, Kotzampassi K. The impact of weight loss on depression status in obese individuals subjected to intragastric balloon treatment. Obesity Surgery. 2013;23(5):669-75. doi: 10.1007/s11695-012-0855-1.
- Мельникова Е. В., Бабенко А. Ю., Неймарк А. Е. Влияние нарушения пищевого поведения на компенсацию гликемии и снижение массы тела при разных подходах к терапии// Конгресс «Эндокринология Северо-запада России 2015» 18-20 июня 2015 г., Санкт-Петербург - тезисы докладов: с. 37.
- Bhasker A. G. et al. Predictors of Remission of T2DM and Metabolic Effects after Laparoscopic Roux-en-y Gastric Bypass in Obese Indian Diabetics - a 5-Year Study // Obes. Surg. 2014.
- Chattranukulchai Shantavasinkul P. et al. Predictors of weight regain in patients who underwent Roux-en-Y gastric bypass surgery // 2016.
- Lars Sjöström et al. Lifestyle, Diabetes, and Cardiovascular Risk Factors 10 Years after Bariatric Surgery // N. Engl. J. Med. 2004. С. 2683-2693.
- Wood G. C. et al. Association of DiaRem Score With Cure of Type 2 Diabetes Following Bariatric Surgery // JAMA Surg. 2016. Т. 151. № 8. С. 779.
- Brandenburg D. History and diagnostic significance of C-peptide.Exp Diabetes Res 2008: 576862
- Schauer PR, Burguera B, Ikramuddin S, Cottam D, Gourash W, Hama G, et al. Effect of laparoscopic Roux-en Y gastric bypass on type 2 diabetes mellitus. Ann Surg. 2003; 238:467-84. discussion 84-5.
- Aarts, E. O., Janssen, J., Janssen, I. M. C., Berends, F. J., Telting, D., & De Boer, H. (2013). Preoperative fasting plasma C-peptide level may help to predict diabetes outcome after gastric bypass surgery. Obesity Surgery, 23(7), 867-873.
Для цитирования :
Тихоненко Е.В., Бабенко А.Ю., Неймарк А.Е., Корнюшин С.В., Боярская И.А. ПРЕДИКТОРЫ СНИЖЕНИЯ ВЕСА И РЕМИССИИ САХАРНОГО ДИАБЕТА ПОСЛЕ УСТАНОВКИ ВНУТРИЖЕЛУДОЧНОГО БАЛЛОНА И ДРУГИХ БАРИАТРИЧЕСКИХ ВМЕШАТЕЛЬСТВ. Экспериментальная и клиническая гастроэнтерология. 2017;143(07):82-88
Загрузить полный текст
ОГЛАВЛЕНИЯ ВЫПУСКОВ
Контакты
Submission of the manuscript is online via e-mail
ecgarticle@gmail.com or
cholerez@mail.ru
Editorial Correspondence e-mail
gastrossr@gmail.com
Publishing, Subscriptions, Sales and Advertising, Correspondence e-mail
journal@cniig.ru
Tel: +7 917 561 9505
COVID-19
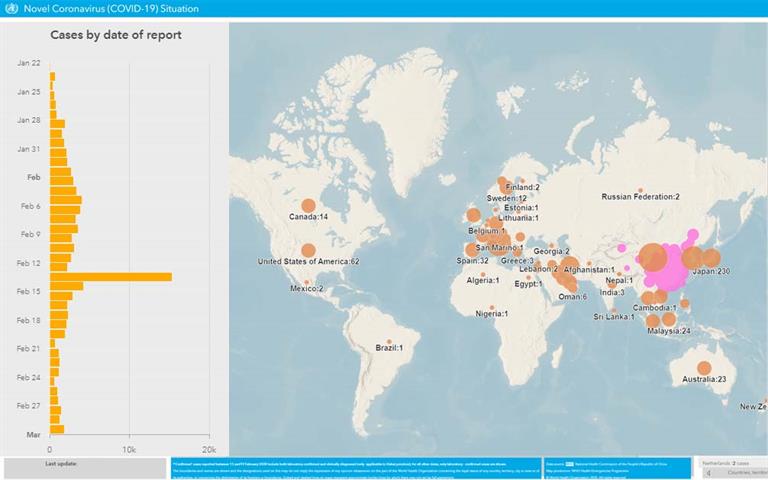
Coronavirus disease (COVID-19) Situation dashboard
This interactive dashboard/map provides the latest global numbers and numbers by country of COVID-19 cases on a daily basis.
Scimago Journal & Country Rank